

Successful use of avacopan in a case of ANCA-associated vasculitis with treatment-resistant medium-sized vessel involvement
- PMID: 39849229
- PMCID: PMC12307840
- DOI: 10.1007/s13730-025-00965-8
Successful use of avacopan in a case of ANCA-associated vasculitis with treatment-resistant medium-sized vessel involvement
Abstract
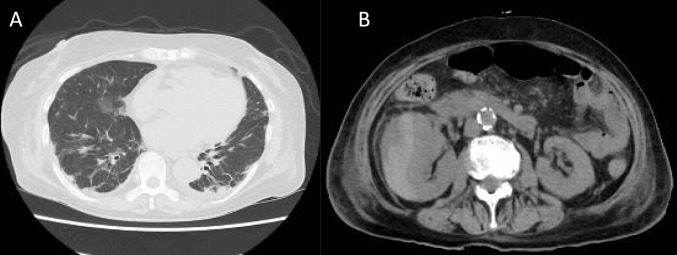
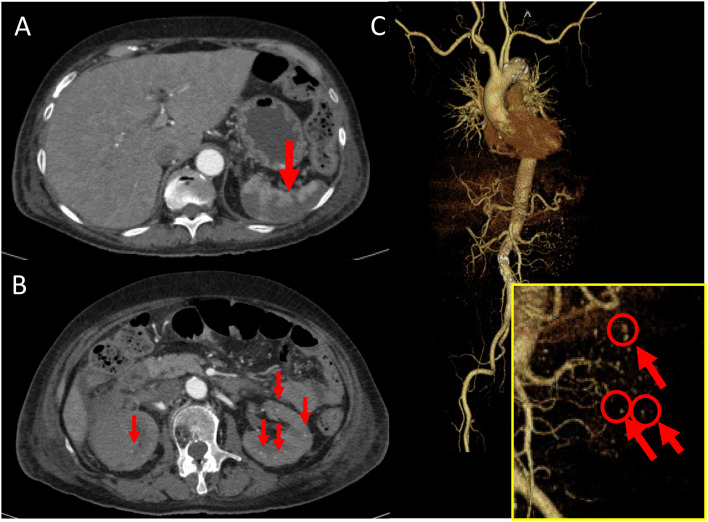
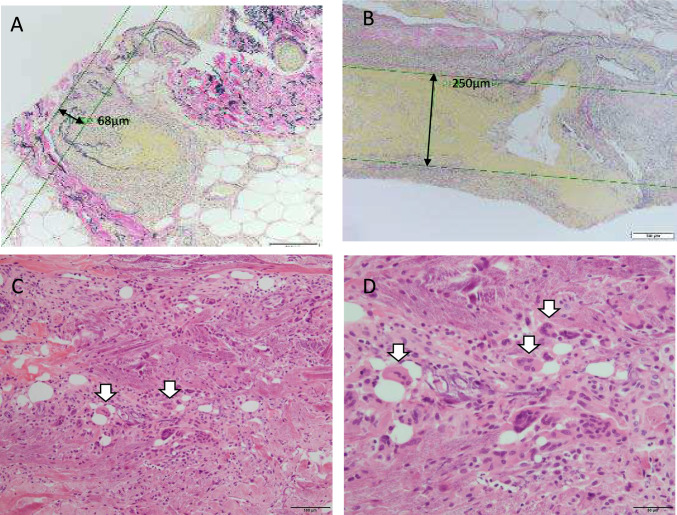
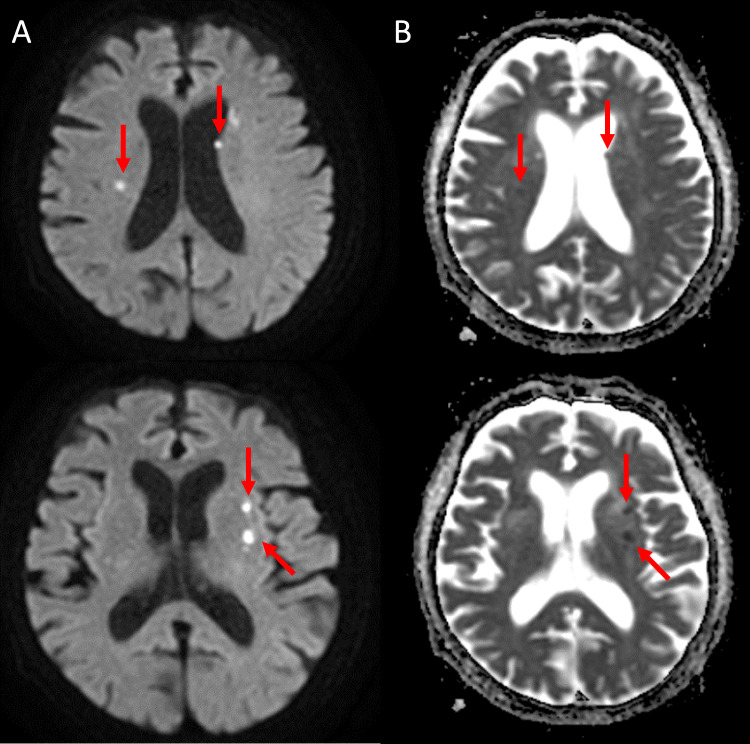
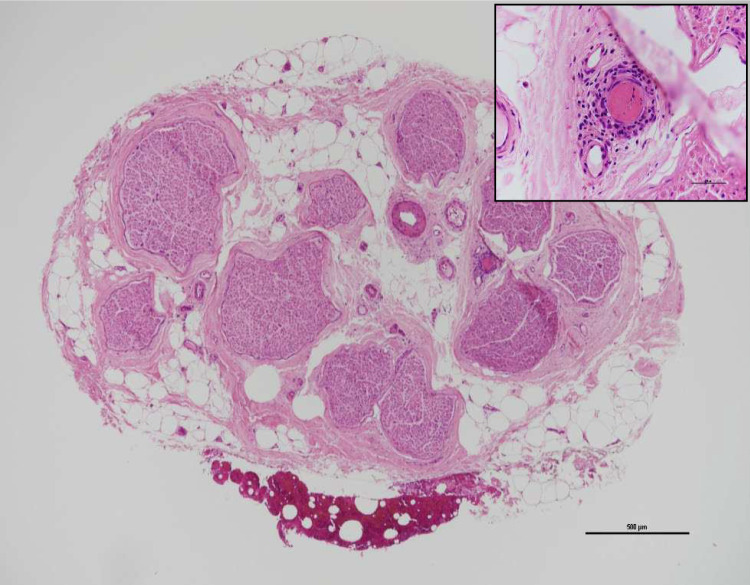
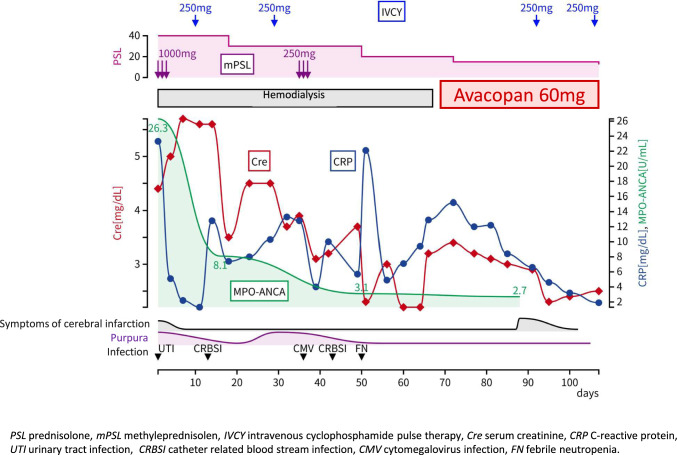
We report the case of a 75-year-old woman who presented with fever, right back pain, paresthesia in the right extremities, erythema, purpura, and nodules. She had previously initiated dialysis due to rapidly progressive glomerulonephritis and was transferred to our hospital. Imaging studies revealed multiple cerebral and splenic infarcts and hemorrhage encapsulating the right kidney, likely due to microaneurysms in multiple renal arteries. High MPO-ANCA titers were observed, and a skin biopsy revealed granulomatous inflammation affecting medium-sized vessels, leading to a diagnosis of granulomatosis with polyangiitis (GPA) and ANCA-associated vasculitis (AAV) involving medium-sized vessels. Treatment began with intravenous pulse steroid therapy (methylprednisolone 1000 mg/day) and subsequent oral prednisolone (PSL) 40 mg (about 0.8 mg/kg) and intravenous cyclophosphamide (IVCY) at 250 mg. While her symptoms improved, she developed severe infections, including candidemia and febrile neutropenia. Consequently, we combined PSL with the C5a receptor antagonist avacopan, which allowed for PSL tapering and stabilized her disease. This case is significant as no previous reports of avacopan's efficacy in AAV with medium-sized vessel involvement suggest its potential effectiveness in such cases.
Keywords: ANCA-associated vasculitis with medium-sized vessel involvement; Avacopan; Granulomatosis with polyangiitis; Microaneurysms in renal arteries.
© 2025. The Author(s), under exclusive licence to Japanese Society of Nephrology.
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no conflicts of interest. Ethical approval: Written informed consent was obtained from the patient for the treatment and for the publication of this case report.
Figures
Similar articles
-
Successful treatment of MPO-ANCA positive crescentic IgA nephropathy/IgA vasculitis with nephritis potentially triggered by a COVID-19 vaccine in a young adult female using corticosteroids, rituximab, and avacopan.CEN Case Rep. 2025 Aug;14(4):626-632. doi: 10.1007/s13730-025-00991-6. Epub 2025 Apr 9. CEN Case Rep. 2025. PMID: 40202709 Free PMC article.
-
Antineutrophil cytoplasmic antibodies in infective endocarditis: a case report and systematic review of the literature.Clin Rheumatol. 2022 Oct;41(10):2949-2960. doi: 10.1007/s10067-022-06240-w. Epub 2022 Jun 23. Clin Rheumatol. 2022. PMID: 35732985 Free PMC article.
-
Gastric presentation (vasculitis) mimics a gastric cancer as initial symptom in granulomatosis with polyangiitis: a case report and review of the literature.Rheumatol Int. 2015 Nov;35(11):1925-9. doi: 10.1007/s00296-015-3334-x. Epub 2015 Aug 7. Rheumatol Int. 2015. PMID: 26248531
-
Granulomatosis with polyangiitis with rapidly progressive glomerulonephritis treated with a multipronged approach-a case based review.CEN Case Rep. 2025 Aug;14(4):567-572. doi: 10.1007/s13730-024-00959-y. Epub 2024 Dec 20. CEN Case Rep. 2025. PMID: 39704740 Free PMC article. Review.
-
Significance of clinical-immunological patterns and diagnostic yield of biopsies in microscopic polyangiitis and granulomatosis with polyangiitis.J Intern Med. 2024 May;295(5):651-667. doi: 10.1111/joim.13777. Epub 2024 Mar 11. J Intern Med. 2024. PMID: 38462959
References
-
- Nakazawa D, Masuda S, Tomaru U, Ishizu A. Pathogenesis and therapeutic interventions for ANCA-associated vasculitis. Nat Rev Rheumatol. 2019;15:91–101. - PubMed
-
- Hellmich B, Sanchez-Alamo B, Schirmer JH, Berti A, Blockmans D, Cid MC, Holle JU, Hollinger N, Karadag O, Kronbichler A, Little MA, Luqmani RA, Mahr A, Merkel PA, Mohammad AJ, Monti S, Mukhtyar CB, Musial J, Price-Kuehne F, Segelmark M, Teng YKO, Terrier B, Tomasson G, Vaglio A, Vassilopoulos D, Verhoeven P, Jayne D. EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update. Ann Rheum Dis. 2024;83:30–47. - PubMed
-
- Jayne DRW, Merkel PA, Schall TJ, Bekker P, ADVOCATE Study Group. Avacopan for the treatment of ANCA-associated vasculitis. N Engl J Med. 2021;384:599–609. - PubMed
-
- Isoda K, Nuri K, Shoda T, Kotani T, Satoh T, Ishida S, Takeuchi T, Makino S, Hanafusa T. Microscopic polyangiitis complicated with cerebral infarction and hemorrhage: a case report and review of literature. Nihon Rinsho Meneki Gakkai Kaishi. 2010;33:111–5. - PubMed
-
- Yamagata K, Usui J, Saito C, Yamaguchi N, Hirayama K, Mase K, Kobayashi M, Koyama A, Sugiyama H, Nitta K, Wada T, Muso E, Arimura Y, Makino H, Matsuo S. ANCA-associated systemic vasculitis in Japan: clinical features and prognostic changes. Clin Exp Nephrol. 2012;16:580–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
