

Prognostic significance of peripheral blood biomarkers in patients with advanced renal cell carcinoma treated with nivolumab and ipilimumab-a polish multicenter, observational study
- PMID: 39849293
- PMCID: PMC11759459
- DOI: 10.1007/s10238-024-01544-4
Prognostic significance of peripheral blood biomarkers in patients with advanced renal cell carcinoma treated with nivolumab and ipilimumab-a polish multicenter, observational study
Abstract
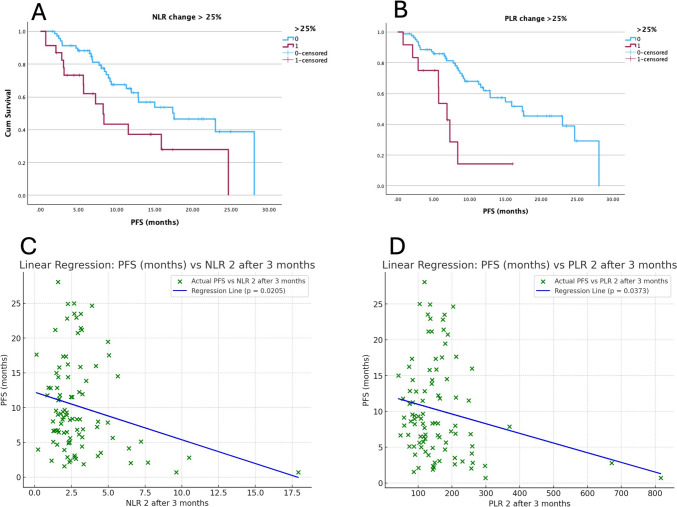
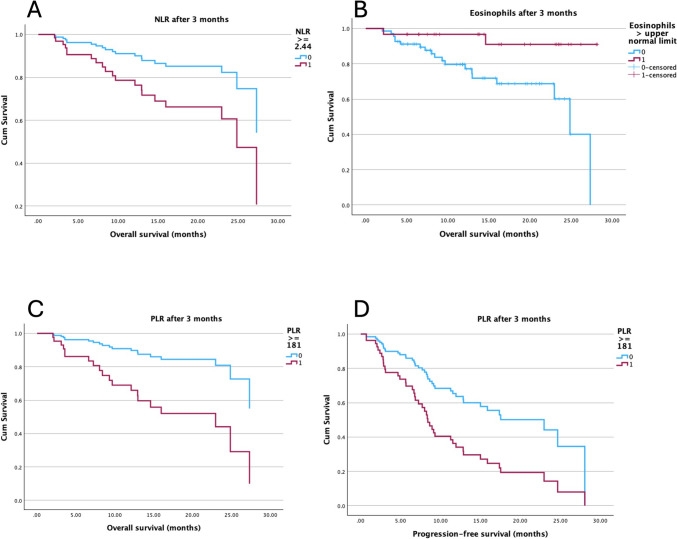
Immune checkpoint inhibitors have improved the treatment of metastatic renal cell carcinoma (RCC), with the combination of nivolumab (NIVO) and ipilimumab (IPI) showing promising results. However, not all patients benefit from these therapies, emphasizing the need for reliable, easily assessable biomarkers. This multicenter study involved 116 advanced RCC patients treated with NIVO + IPI across nine oncology centers in Poland. Blood markers such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR), eosinophils, and monocytes were assessed at baseline, after three months, and before disease progression (PD). The prognostic significance of these parameters was analyzed using linear regression, Kaplan-Meier survival analysis, and Cox regression models. After a median follow-up of 11.8 months, the progression-free survival (PFS) was 12.8 months (95% confidence interval [CI] 5.7-28.1), while the overall survival (OS) was 27.3 months (95% CI 16-not reached). Patients with an NLR increase of ≥ 25% had a PFS of 8.2 (3.1-24.7) months compared to 17.5 (8.6-28.1) months in those with a rise in < 25% (p = 0.015). Similarly, a ≥ 25% increase in PLR was linked to a PFS of 6.8 (2.8-8.3) months compared to 17.4 (8.4-28.1) months (p < 0.001). Multivariate analysis confirmed PLR as an independent predictor of PFS (HR 2.9, 95% CI 1.5-5.6, p = 0.001), while elevated eosinophil levels were associated with a reduced risk of death (HR 0.2, 95% CI 0.04-0.9, p = 0.05). No other analysis was statistically significant. NLR, PLR, and eosinophil levels may serve as valuable biomarkers for predicting treatment response in RCC patients receiving NIVO + IPI.
Keywords: Eosinophils; Immune checkpoint inhibitors; Lymphocyte-to-monocyte ratio; Neutrophil-to-lymphocyte ratio; Platelet-to-lymphocyte ratio; Prognostic factors; Renal cell carcinoma.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: RPM has received travel grants from Accord, BMS, MSD, and lecture fees from Astra Zeneca, BMS, GSK, Novartis, Roche, MSD; AD has received travel grants and lecture fees from Roche, BMS, Janssen, Molteni, MSD, Accord; AGW has received travel grants and lecture fees from Roche, Novaris, Lili, Astellas, Pfizer, Amgen, Swixx, Pierre Fabre, Egis, BMS, MSD; JC has received lecture fees from BMS; NVV has no financial interests; DTM has received travel grants and lecture fees from MSD, Pierre Fabre, BMS, Novartis, Pfizer; JD has received travel grants and lecture fees from Amgen, AstraZeneca, BMS, MSD, Novartis, Nutricia; AR has received travel grants and lecture fees from Roche, BMS, Ipsen, Pfizer, Novartis, Gilead, MSD; AB has received travel grants and lecture fees from BMS, MSD, Astellas, Merck, Servier, Astra Zeneca, Pfizer; MS has received travel grants and lecture fees from Roche, BMS, Janssen, MSD, Amgen, Astellas., Ipsen, Pfizer, Novartis, Gilead; AGU has received travel grants from GSK, Lilly, Astra Zeneca, Gilead, Accord, and lecture fees from Astra Zeneca. JW has no financial interests; PB has received travel grants, lecture fees, and advisory boards from AstraZeneca, MSD, GSK, Pharma; ŁS has received travel grants from BMS, Accord; MP has received travel grants and lecture fees from AstraZeneca, Roche, Novartis, Elli Lilly, Janssen, Gilead, and Amgen. Ethical approval: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Jagiellonian University Medical College (approval number 118.0043.1.115.2024, dated April 19, 2024). Consent to participate: Informed, institutional consent was obtained from all individual participants included in the study before starting treatment.
Figures
References
-
- Powles T, Albiges L, Bex A, et al. Renal cell carcinoma: ESMO clinical practice guideline for diagnosis, treatment and follow-up 5 behalf of the ESMO guidelines committee. Ann Oncol. 2024;35:692–706. - PubMed
-
- Singer EA, Rumble RB, Van Veldhuizen PJ. Management of metastatic clear cell renal cell carcinoma: ASCO guideline Q&A. JCO Oncol Pract. 2023;19:127–31. - PubMed
-
- Wysocki PJ, Chłosta P, Chrzan R, et al (2022) WYTYCZNE POSTĘPOWANIA DIAGNOSTYCZNO-TERAPEUTYCZNEGO Zalecenia postępowania diagnostyczno-terapeutycznego w raku nerkowokomórkowym-aktualizacja Polish Society of Clinical Oncology and Polish Urological Association guidelines for the diagnosis and treatment of renal cell cancer-update. 6:424–457
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
