

A systematic review of outcomes reported in studies to optimise the medication use of patients at hospital discharge
- PMID: 39849488
- PMCID: PMC11758755
- DOI: 10.1186/s12913-024-12024-6
A systematic review of outcomes reported in studies to optimise the medication use of patients at hospital discharge
Abstract
Introduction: Care transitions, specifically hospital discharge, hold a risk for drug-related problems and medication errors. Effective interventions that optimise medication use during and after transitions are needed, yet there is no standardisation of the outcomes. This literature review aimed at collecting outcomes from studies investigating how to optimise medication use of patients following hospital discharge, and to categorise them, as a first step in the development of a core outcome set.
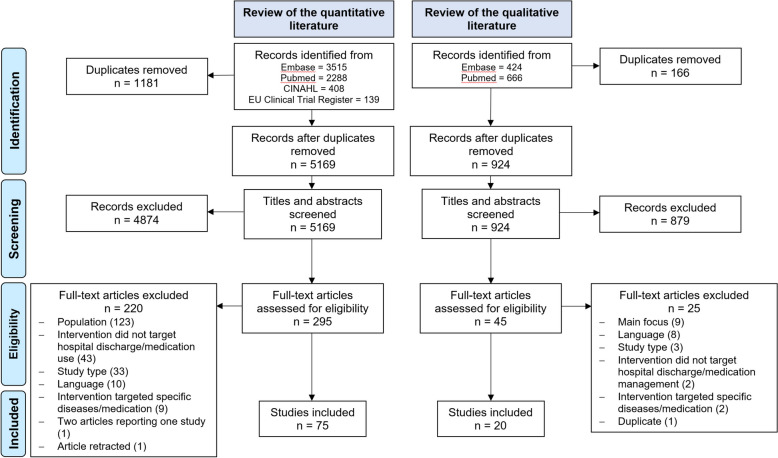
Methods: We systematically reviewed quantitative and qualitative literature using Embase, PubMed, CINAHL and the EU Clinical Trial Register databases. Studies investigating the optimisation of medication use following hospital discharge were eligible. The quantitative literature review specifically included trials and protocols that evaluated the effect of an intervention for patients ≥ 65 years or multimorbid / polypharmacy patients, as they are at high risk of drug-related problems. The qualitative literature review focused on the patients' and healthcare professionals' views. Outcomes were summarised into unique outcome terms and categorised using an adapted version of the OMERACT filter 2.0.
Results: The review included 75 quantitative and 20 qualitative studies. The interventions investigated in the quantitative literature mostly had multiple components performed either pre- or post-discharge. Sixty percent of the qualitative studies addressed the views of healthcare professionals, 40% the views of patients, and only one study addressed both. A median of 5 outcomes (range 1-17) were reported in the quantitative studies. In total, 91 unique outcomes were identified from the quantitative or qualitative literature, or both (73, 12 and 6 outcomes, respectively). Outcomes were categorised into five domains: 'medication' (n = 32 outcomes), 'economic impact/resource use' (n = 26), 'life impact' (n = 16), 'pathophysiological manifestations' (n = 15) and 'death' (n = 2). The top 5 most frequently measured outcomes in quantitative studies were number of readmissions (n = 54/75, 72%), mortality (n = 30/75, 40%), number of emergency department visits (n = 26/75, 35%), number of outpatient physician visits (n = 12/75, 16%), and medication adherence (n = 12/75, 16%).
Discussion and conclusion: This study identified a large number of different outcomes, especially in the domains medication and economic impact/resource use. This heterogeneity impedes the identification of effective interventions and confirms the need for a core outcome set.
Keywords: Continuity of patient care; Core outcome set; Drug therapy; Medication therapy management; Systematic review; Transitional care.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Interventions for improving medication-taking ability and adherence in older adults prescribed multiple medications.Cochrane Database Syst Rev. 2020 May 8;5(5):CD012419. doi: 10.1002/14651858.CD012419.pub2. Cochrane Database Syst Rev. 2020. PMID: 32383493 Free PMC article.
-
Promoting and supporting self-management for adults living in the community with physical chronic illness: A systematic review of the effectiveness and meaningfulness of the patient-practitioner encounter.JBI Libr Syst Rev. 2009;7(13):492-582. doi: 10.11124/01938924-200907130-00001. JBI Libr Syst Rev. 2009. PMID: 27819974
-
Impact of interventions to improve recovery of older adults following planned hospital admission on quality-of-life following discharge: linked-evidence synthesis.Health Soc Care Deliv Res. 2023 Nov;11(23):1-164. doi: 10.3310/GHTY5117. Health Soc Care Deliv Res. 2023. PMID: 38140881
-
Improving inappropriate medication and information transfer at hospital discharge: study protocol for a cluster RCT.Implement Sci. 2018 Dec 27;13(1):155. doi: 10.1186/s13012-018-0839-1. Implement Sci. 2018. PMID: 30591069 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
References
-
- Foulon V, Wuyts J, Desplenter F, Spinewine A, Lacour V, Paulus D, et al. Problems in continuity of medication management upon transition between primary and secondary care: patients’ and professionals’ experiences. Acta Clin Belg. 2018;June:1–9. 10.1080/17843286.2018.1483561. - PubMed
-
- Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians. JAMA. 2007;297:831–41. 10.1001/jama.297.8.831. - PubMed
-
- Griese-Mammen N, Schulz M, Böni F, Hersberger KE. Medication Review and Medication Reconciliation. The Pharmacist Guide to Implementing Pharmaceutical Care, Cham: Springer International Publishing; 2019, p. 69–87. 10.1007/978-3-319-92576-9_7.
-
- World Health Organization. Medication safety in transitions of care [Web page]. [last accessed 2024 Dec 4]. Available from: https://www.who.int/publications/i/item/WHO-UHC-SDS-2019.9.
-
- Donaldson LJ, Kelley ET, Dhingra-Kumar N, Kieny MP, Sheikh A. Medication Without Harm: WHO’s Third Global Patient Safety Challenge. The Lancet. 2017;389:1680–1. 10.1016/S0140-6736(17)31047-4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
