

WT1-mRNA dendritic cell vaccination of patients with glioblastoma multiforme, malignant pleural mesothelioma, metastatic breast cancer, and other solid tumors: type 1 T-lymphocyte responses are associated with clinical outcome
- PMID: 39849594
- PMCID: PMC11755790
- DOI: 10.1186/s13045-025-01661-x
WT1-mRNA dendritic cell vaccination of patients with glioblastoma multiforme, malignant pleural mesothelioma, metastatic breast cancer, and other solid tumors: type 1 T-lymphocyte responses are associated with clinical outcome
Erratum in
-
Correction: WT1-mRNA dendritic cell vaccination of patients with glioblastoma multiforme, malignant pleural mesothelioma, metastatic breast cancer, and other solid tumors: type 1 T-lymphocyte responses are associated with clinical outcome.J Hematol Oncol. 2025 Mar 19;18(1):34. doi: 10.1186/s13045-025-01683-5. J Hematol Oncol. 2025. PMID: 40108626 Free PMC article. No abstract available.
Abstract
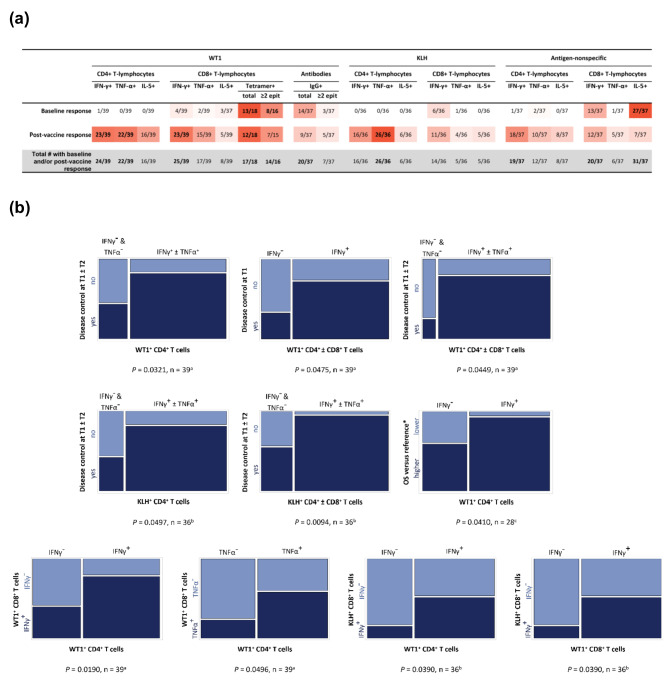
Cell therapies, including tumor antigen-loaded dendritic cells used as therapeutic cancer vaccines, offer treatment options for patients with malignancies. We evaluated the feasibility, safety, immunogenicity, and clinical activity of adjuvant vaccination with Wilms' tumor protein (WT1) mRNA-electroporated autologous dendritic cells (WT1-mRNA/DC) in a single-arm phase I/II clinical study of patients with advanced solid tumors receiving standard therapy. Disease status and immune reactivity were evaluated after 8 weeks and 6 months. WT1-mRNA/DC vaccination was feasible in all patients, except one. Vaccination was well tolerated without evidence of systemic toxicity. The disease control rate and overall response rate among a total of 39 evaluable patients were 74.4% and 12.8%, respectively. Median overall survival (OS) was 43.7 months among 13 patients with glioblastoma multiforme, 41.9 months among 12 patients with metastatic breast cancer, and 48.8 months among 10 patients with malignant pleural mesothelioma, comparing favourably with historical controls reported in the literature. OS was longer in patients with stable disease at 8 weeks and disease control at 6 months versus patients without disease control at either time point. Disease control and higher OS were associated with antigen-specific type 1 CD4+ and/or CD8+ T-lymphocyte responses, mainly induced by WT1-mRNA/DC vaccination. Antigen-nonspecific type 2 CD8+ T-cell responses were common before WT1-mRNA/DC vaccination but did not show any association with clinical outcome. Collectively, these data indicate that WT1-mRNA/DC vaccination is feasible, safe, and immunogenic and shows clinical activity in patients with advanced solid tumors, suggesting that it has the potential to help improve their survival.
Keywords: Cancer immunotherapy; Clinical trial; Dendritic cell vaccination; Glioblastoma multiforme; Malignant pleural mesothelioma; Metastatic breast cancer; Solid tumors; Type 1 T-lymphocyte response; Wilms’ tumor protein; mRNA.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethics Committee of the Antwerp University Hospital/University of Antwerp (EC 10/40/266) and the Belgian Federal Agency for Medicines and Health Products (FAGG 08 − 0005) and registered at ClinicalTrials.gov (NCT01291420) and EudraCT (2011-000547-24). The sponsor’s protocol code was CCRG 11 − 001. All participants provided informed written consent in accordance with the principles of the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: VFVT and ZNB are coinventors of a now-elapsed patent covering the messenger RNA electroporation technique (Improved Transfection of Eukaryotic Cells with Linear Polynucleotides by Electroporation, WO/2003/000907).
Figures
References
-
- Sugiyama H. Cancer immunotherapy targeting Wilms’ tumor gene WT1 product. Expert Rev Vaccines. 2005;4(4):503–12. - PubMed
-
- Gobbini E, Ezzalfani M, Dieras V, Bachelot T, Brain E, Debled M, et al. Time trends of overall survival among metastatic breast cancer patients in the real-life ESME cohort. Eur J Cancer. 2018;96:17–24. - PubMed
-
- Nelson DB, Rice DC, Niu J, Atay S, Vaporciyan AA, Antonoff M, et al. Long-term survival outcomes of cancer-directed surgery for malignant pleural mesothelioma: propensity score matching analysis. J Clin Oncol. 2017;35(29):3354–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
