

Primary Cutaneous Methotrexate-Associated T-Cell Lymphoproliferative Disorder in the Setting of Autoimmune Disease: A Case Series and Review of the Literature
- PMID: 39851907
- PMCID: PMC11776889
- DOI: 10.1097/DAD.0000000000002905
Primary Cutaneous Methotrexate-Associated T-Cell Lymphoproliferative Disorder in the Setting of Autoimmune Disease: A Case Series and Review of the Literature
Abstract
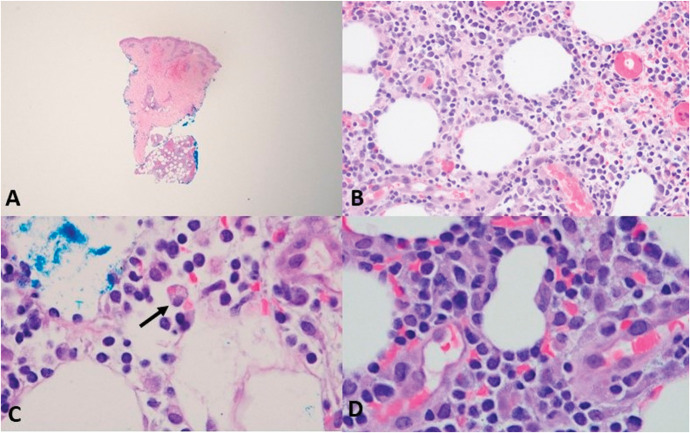
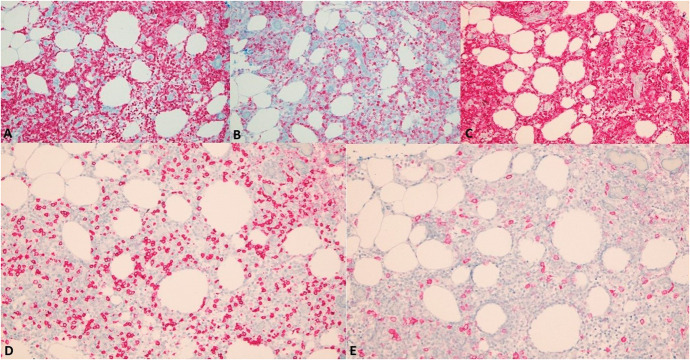
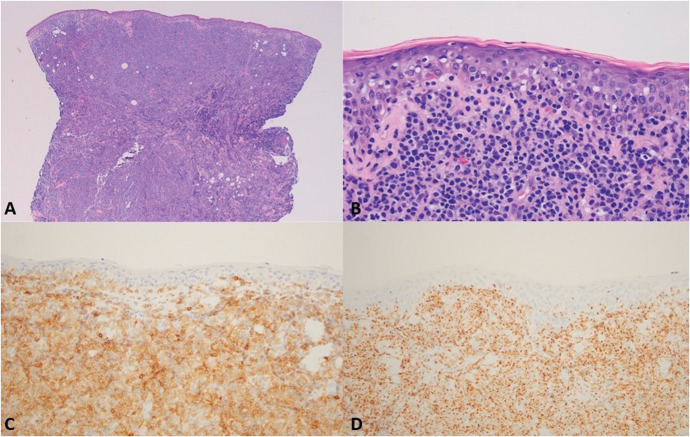
Methotrexate (MTX), an antimetabolite targeting certain autoimmune conditions and various hematologic malignancies, has been associated with iatrogenic lymphoproliferative disease (LPD) primarily of B-cell lineage. Less commonly are T-cell neoplasms where primary skin involvement is considered rare. Three cases were encountered in the medical practice of one of the authors. The patients ranged in age from 38 years to 99 years (2 women and 1 man) with 2 having rheumatoid arthritis and 1 having ankylosing spondylitis. All 3 patients received MTX. The cases included subcutaneous peripheral T-cell lymphoma not otherwise specified (NOS) (1 patient), mycosis fungoides (1 patient), and a primary aggressive epidermotropic cytotoxic T-cell lymphoma (1 patient) that proved to be fatal. One patient had spontaneous regression following MTX withdrawal; she later developed a recurrence while off MTX. Two patients died, 1 of unrelated causes and 1 of lymphoma. Seven previously reported cases included subcutaneous panniculitis-like T-cell lymphoma (2 cases), primary cutaneous CD4+ LPD (2 cases), peripheral T-cell lymphoma (NOS) (1 case), anaplastic large cell lymphoma (1 case), and peripheral T-cell lymphoma localized to fat (1 case). Regression without recurrence occurred in 6 of the 7 patients with MTX withdrawal. The patients were on the MTX for an average of 4 years and had a median age of 61 years with a slight dominance of men over women. Three of the 7 cases showed Epstein-Barr encoding region (EBER) positivity while the 3 cases reported in this series were negative. MTX-associated T-cell LPD involves older patients on long-term MTX where EBER positivity is more frequent than extracutaneous MTX-associated T-cell LPD. A spectrum of classic forms of CTCL is seen with subcutaneous involvement representing a significant percentage of cases. Regression with MTX withdrawal occurs although not in every case.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
Biologics or tofacitinib for people with rheumatoid arthritis naive to methotrexate: a systematic review and network meta-analysis.Cochrane Database Syst Rev. 2017 May 8;5(5):CD012657. doi: 10.1002/14651858.CD012657. Cochrane Database Syst Rev. 2017. PMID: 28481462 Free PMC article.
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.Health Technol Assess. 2006 Nov;10(42):iii-iv, xi-xiii, 1-229. doi: 10.3310/hta10420. Health Technol Assess. 2006. PMID: 17049139
-
Central Nervous System Lymphoproliferative Disorder Secondary to Methotrexate: A Systematic Literature Review and Case Illustration.World Neurosurg. 2023 Nov;179:118-126. doi: 10.1016/j.wneu.2023.08.018. Epub 2023 Aug 12. World Neurosurg. 2023. PMID: 37574195
-
Infliximab and methotrexate in the treatment of rheumatoid arthritis: a systematic review and meta-analysis of dosage regimens.Clin Ther. 2008 Nov;30(11):1939-55. doi: 10.1016/j.clinthera.2008.11.007. Clin Ther. 2008. PMID: 19108784
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
References
-
- Shibusawa M, Kidoguchi K, Tanimoto T. Other iatrogenic immunodeficiency-associated lymphoproliferative disorders. In: Gallamini A, Juweid M, eds. Lymphoma [Internet]. Brisbane, Australia: Exon Publications; 2021. Chapter 4. - PubMed
-
- Tournadre A, D'Incan M, Dubost JJ, et al. . Cutaneous lymphoma associated with Epstein-Barr virus infection in 2 patients treated with methotrexate. Mayo Clin Proc. 2001;76:845–848. - PubMed
-
- Kondo S, Tanimoto K, Yamada K, et al. . Mature T/NK-cell lymphoproliferative disease and Epstein-Barr virus infection are more frequent in patients with rheumatoid arthritis treated with methotrexate. Virchows Arch. 2013;462:399–407. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
