

The Influence of Concurrent Autoimmune Thyroiditis on the Cardiometabolic Consequences of Cabergoline in Postmenopausal Women
- PMID: 39852352
- PMCID: PMC11767027
- DOI: 10.3390/metabo15010009
The Influence of Concurrent Autoimmune Thyroiditis on the Cardiometabolic Consequences of Cabergoline in Postmenopausal Women
Abstract
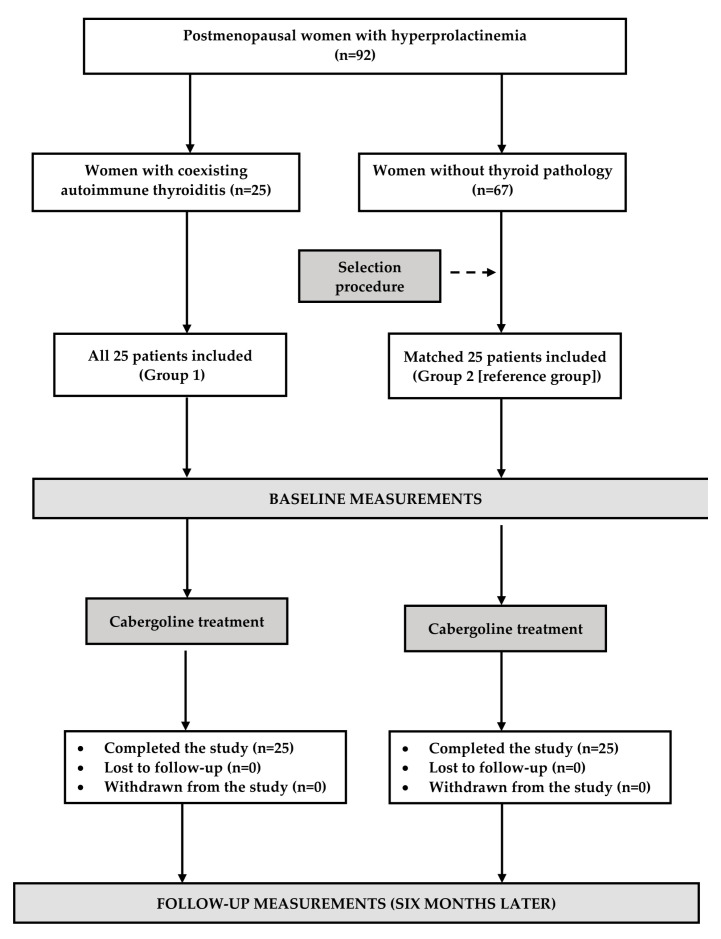
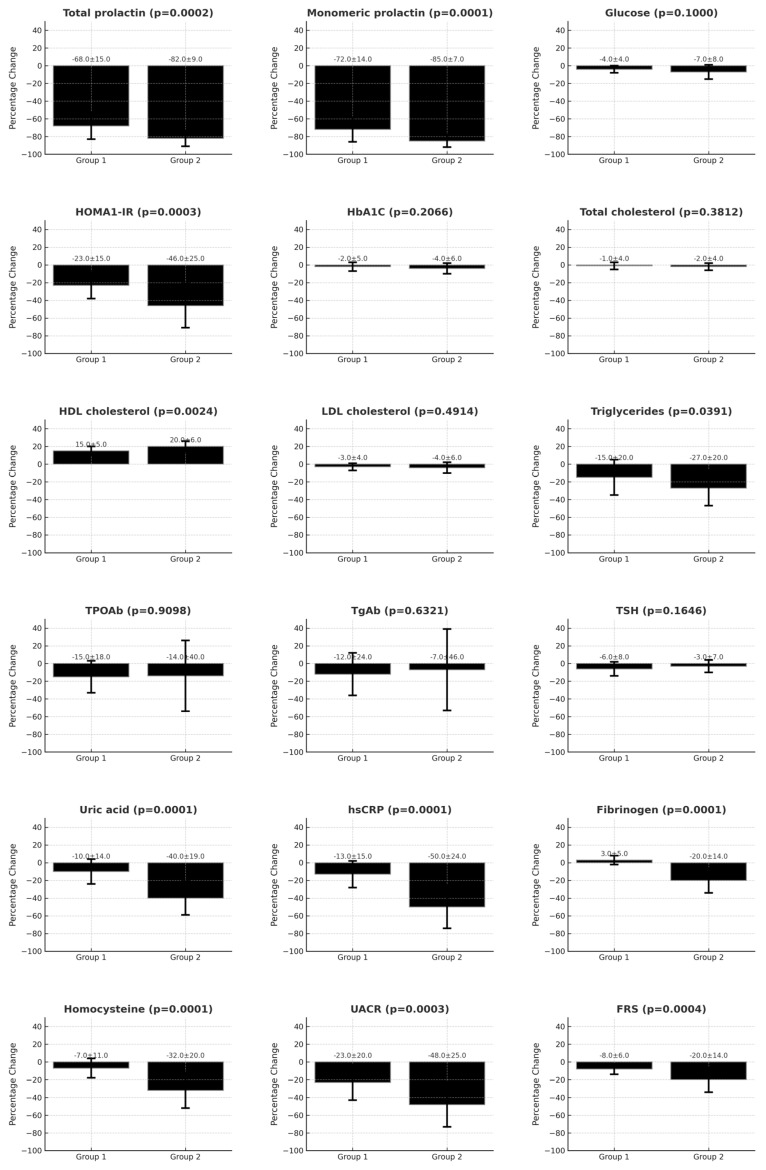
Background: Untreated hyperprolactinemia and autoimmune thyroiditis (Hashimoto's disease) seem to increase cardiometabolic risk. The cardiometabolic effects of cabergoline were less significant in young women with concurrent euthyroid Hashimoto's illness. This study sought to investigate if the detrimental effects of this condition on cabergoline efficacy are also evident in postmenopausal women. Methods: The study comprised 50 postmenopausal women exhibiting increased prolactin levels, with half qualifying for euthyroid Hashimoto's illness. The subjects with thyroid autoimmunity were matched with those without thyroid disease according to age, body mass index, and prolactin levels. In addition to prolactin, we assessed thyroid-stimulating hormone (TSH), thyroid antibodies, and glucose homeostasis markers: fasting glucose, the homeostatic model assessment 1 of insulin resistance ratio (HOMA1-IR), and glycated hemoglobin (HbA1c). Furthermore, we assessed plasma lipids, plasma uric acid levels, high-sensitivity C-reactive protein (hsCRP), fibrinogen, homocysteine, and the urine albumin-to-creatinine ratio (UACR). The decadal cardiovascular risk was assessed with the Framingham Risk Score (FRS). Results: Before therapy, disparities existed among groups in HOMA1-IR, HDL cholesterol, antibody titers, uric acid, hsCRP, fibrinogen, homocysteine, UACR, and FRS. After six months of treatment, cabergoline successfully corrected prolactin levels (both total and monomeric) in women without thyroid disorders. This normalization correlated with decreases in HOMA1-IR, triglycerides, uric acid, hsCRP, fibrinogen, homocysteine, UACR, and FRS, as well as an elevation in HDL cholesterol. In women diagnosed with Hashimoto's disease, cabergoline's effects were limited to a reduction in prolactin levels, HOMA1-IR, and UACR, as well as an elevation in HDL cholesterol, with these alterations being less pronounced compared to women without thyroid illness. Conclusions: The cardiometabolic benefits of cabergoline were associated with the degree of prolactin concentration reduction. In women diagnosed with Hashimoto's disease, connections were noted between baseline levels and treatment-induced alterations in hsCRP. These data indicate that concurrent euthyroid autoimmune thyroiditis mitigates the cardiometabolic consequences of cabergoline.
Keywords: insulin sensitivity; lactotroph; postmenopause; prolactin excess; thyroid autoimmunity.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Autoimmune Thyroiditis Attenuates Cardiometabolic Effects of Cabergoline in Young Women With Hyperprolactinemia.J Clin Pharmacol. 2023 Aug;63(8):886-894. doi: 10.1002/jcph.2245. Epub 2023 May 8. J Clin Pharmacol. 2023. PMID: 37042432
-
Vitamin D Status Determines Cardiometabolic Effects of Cabergoline in Women with Elevated Prolactin Levels: A Pilot Study.Nutrients. 2023 May 14;15(10):2303. doi: 10.3390/nu15102303. Nutrients. 2023. PMID: 37242186 Free PMC article.
-
Cardiometabolic Effects of Cabergoline and Combined Oral Contraceptive Pills in Young Women with Hyperprolactinemia: A Pilot Study.J Clin Med. 2023 Apr 29;12(9):3208. doi: 10.3390/jcm12093208. J Clin Med. 2023. PMID: 37176648 Free PMC article.
-
Association of Hashimoto's thyroiditis and thyroid cancer.Curr Opin Oncol. 2015 Jan;27(1):21-5. doi: 10.1097/CCO.0000000000000150. Curr Opin Oncol. 2015. PMID: 25390557 Review.
-
Hashimoto's Encephalopathy: Case Series and Literature Review.Curr Neurol Neurosci Rep. 2023 Apr;23(4):167-175. doi: 10.1007/s11910-023-01255-5. Epub 2023 Feb 28. Curr Neurol Neurosci Rep. 2023. PMID: 36853554 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
