

Treatment Patterns and Economic Burden of Ulcerative Colitis in Japan: A Retrospective Claims Analysis
- PMID: 39853657
- PMCID: PMC11868343
- DOI: 10.1007/s12325-024-03096-1
Treatment Patterns and Economic Burden of Ulcerative Colitis in Japan: A Retrospective Claims Analysis
Abstract
Introduction: This retrospective claims analysis characterized contemporary ulcerative colitis (UC) treatment patterns and investigated the economic burden of UC in Japan.
Methods: This study used anonymized claims data in the Medical Data Vision database. Patients were included if they had a confirmed UC diagnosis and ≥ 1 claim of systemic treatment for UC (index date) between June 2018 and December 2022, in addition to continuous enrollment for ≥ 6 months before and ≥ 12 months after the index date. Patients were excluded if they were aged < 18 years at index or if they had claimed systemic UC treatment during the pre-index period, had a confirmed diagnosis of Crohn's or Behçet's disease, or had a record of colectomy during the pre-index period. Outcomes of interest were treatment patterns, healthcare resource utilization (HCRU), and UC-related costs per person per month (PPPM). Further exploratory analyses were conducted to understand whether real-world treatment patterns with conventional therapy were optimally aligned with guideline recommendations. Two definitions of suboptimal treatment with conventional therapies were identified: prolonged treatment with corticosteroids (i.e., consecutive use for > 90 days) and corticosteroid cycling (i.e., three or more ≥ 30-day corticosteroid courses over 1 year, with a ≥ 60-day gap between courses).
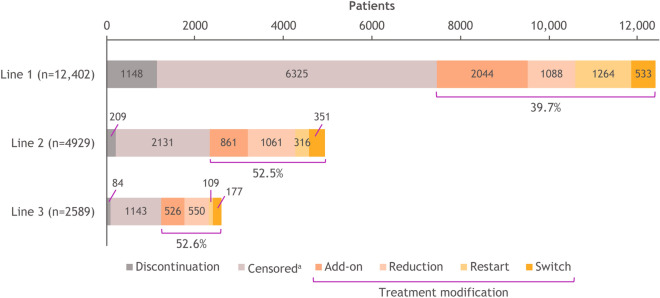
Results: Overall, 15,429 patients were included. The most frequently observed class of first-line treatment was 5-aminosalicylic acid monotherapy (75.0%); treatment modification was observed in 39.7% of patients. Within 1 year of follow-up, patients had a mean (SD) of 9.8 (6.8) outpatient visits, and a hospital stay was reported in 23.9% of patients. Mean total cost PPPM was ¥76,374. Of patients with ≥ 1 course of corticosteroids, 39.8% received suboptimal treatment with conventional therapies. HCRU and total costs were higher for patients with versus without suboptimal treatment with conventional therapies.
Conclusions: Japanese patients with UC would benefit from treatment options that can reduce costs, HCRU, and suboptimal treatment with conventional therapies.
Keywords: Claims analysis; Corticosteroid; Health care costs; Inflammatory bowel disease; Japan; Observational study; Ulcerative colitis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Shingo Kato received honoraria from AbbVie, Janssen Pharmaceutical K.K., Kissei, Mitsubishi Tanabe, and Takeda. Bruno Casaes Teixeira, Thomas Laurent, Yoshiyuki Yamada, Kiran Dave, Shweta Shah, and Hyunchung Kim are employees and/or shareholders of Bristol Myers Squibb. Ethical Approval: This real-world, retrospective, observational study used anonymized patient data from June 2018 to December 2022, obtained from Medical Data Vision, a hospital-based claims database (Medical Data Vision, Tokyo, Japan) that covers approximately 42 million patients across 474 acute care hospitals in Japan. As all data were anonymized, requirements for ethics approval and informed consent under the Ethical Guidelines for Epidemiological Research in Japan do not apply to this study. Permission was obtained to access and use data by Medical Data Vision.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
