

Factors associated with uptake and acceptability of cervical cancer screening among female sex workers in Northeastern Uganda: A cross-sectional study
- PMID: 39854583
- PMCID: PMC11759397
- DOI: 10.1371/journal.pone.0312988
Factors associated with uptake and acceptability of cervical cancer screening among female sex workers in Northeastern Uganda: A cross-sectional study
Abstract
Background: Cervical cancer screening program in Uganda is opportunistic and focuses mainly on women aged 25-49 years. Female sex workers (FSWs) are at increased risk of developing invasive cervical cancer. There is limited data regarding the uptake and acceptability of cervical cancer screening among FSWs in Uganda. This study aimed at identifying factors associated with uptake and acceptability of cervical cancer screening among FSWs in Eastern Uganda.
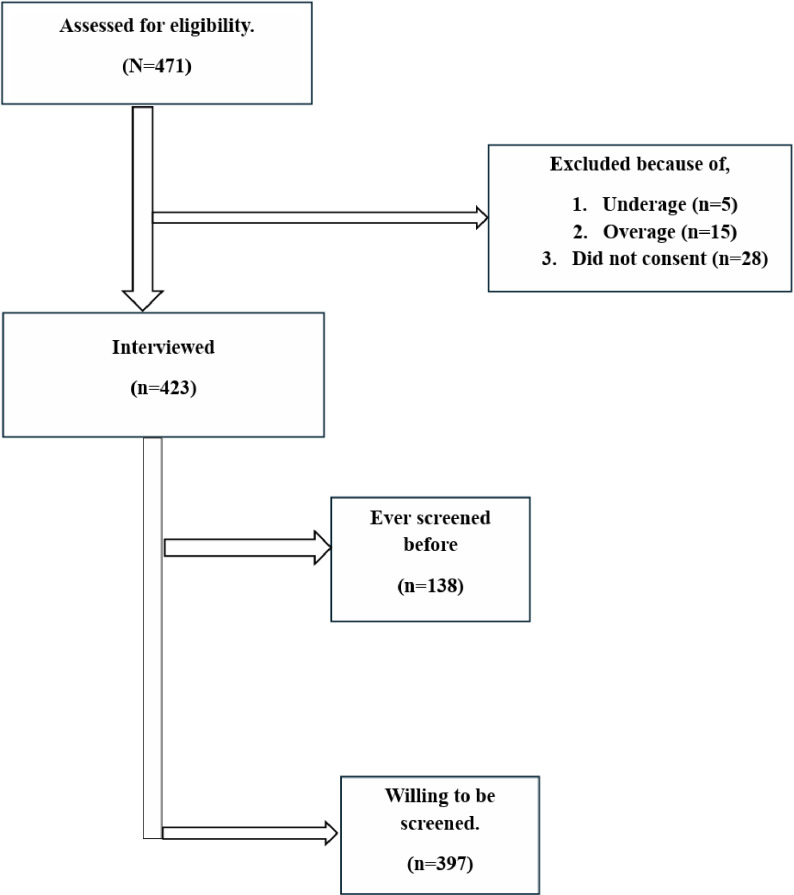
Methods: This was a cross-sectional study conducted among 423 FSWs aged 18-49 years attending care at six health facilities serving Key Populations (FSWs, Men who have sex with men, transgender people, people who inject drugs and people in prisons) in the Teso sub-region. Data was collected using structured investigator administered questionnaire and analyzed using Stata statistical software version 15.0 (Stata Corp, Texas, USA). The primary outcome was uptake of cervical cancer screening measured as the proportion of female sex workers who have ever been screened for cervical cancer. Chi-square test was used to compare the differences in uptake of cervical cancer screening by HIV status. Modified Poisson regression model with a robust variance estimator was used to determine association between the outcome variables and selected independent variables including demographic characteristics. Prevalence ratios (PR) with accompanying 95% confidence intervals have been reported. Statistical significance was considered at two-sided p-values ≤ 0.05.
Results: The mean age of the participants was 28.1 (±SD = 6.6) years. The self-reported HIV prevalence was 21.5% (n = 91). There were 138 (32.6%) participants who had ever been screened for cervical cancer (uptake), while 397 (93.9%) were willing to be screened (acceptability). There was a significant difference in cervical cancer screening uptake between women living with HIV (WLHIV) and those who were HIV negative, 59.3% vs 26.9% respectively (P < 0.001). The significant factors associated with uptake of cervical cancer screening included living with HIV, adjusted prevalence ratio (aPR) = 1.53 (95%CI: 1.15-2.07), increasing number of biological children, aPR = 1.14 (1.06-1.24) living near a private not for profit (PNFP) facility, aPR = 2.84 (95% CI; 1.68-4.80) and availability of screening services at the nearest health facility, aPR = 1.83 (95% CI, 1.30-2.57). Factors significantly associated with acceptability of cervical cancer screening included being 40 years or older, aPR = 1.22 (95%CI: 1.01-1.47), having a family history of cervical cancer, aPR = 1.05 (1.01-1.10), and living near a PNFP facility, aPR = 1.17 (95% CI, 1.09-1.27) and having ever screened before, aPR = 0.92 (0.86-0.98).
Conclusion: Female sex workers living with HIV are more likely to screen for cervical cancer than the HIV negative clients. Cervical cancer screening uptake is relatively low among the female sex workers. However, majority of the FSWs are willing to be screened for cervical cancer if the services are provided in the nearby healthcare facilities. There is need to make cervical cancer screening services available to all eligible women especially the female sex workers and integrate the services with sexual reproductive health services in general and not just HIV/ART clinics services.
Copyright: © 2025 Opito et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- The Global Cancer Observatory. Uganda fact sheet [Internet]. International Agency for Research on Cancers. 2024. [cited 2024 Sep 14]. Available from: https://gco.iarc.who.int/media/globocan/factsheets/populations/800-ugand...
-
- World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva: World Health Organization; 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
