

A multimodal transformer system for noninvasive diabetic nephropathy diagnosis via retinal imaging
- PMID: 39856403
- PMCID: PMC11759696
- DOI: 10.1038/s41746-024-01393-1
A multimodal transformer system for noninvasive diabetic nephropathy diagnosis via retinal imaging
Abstract
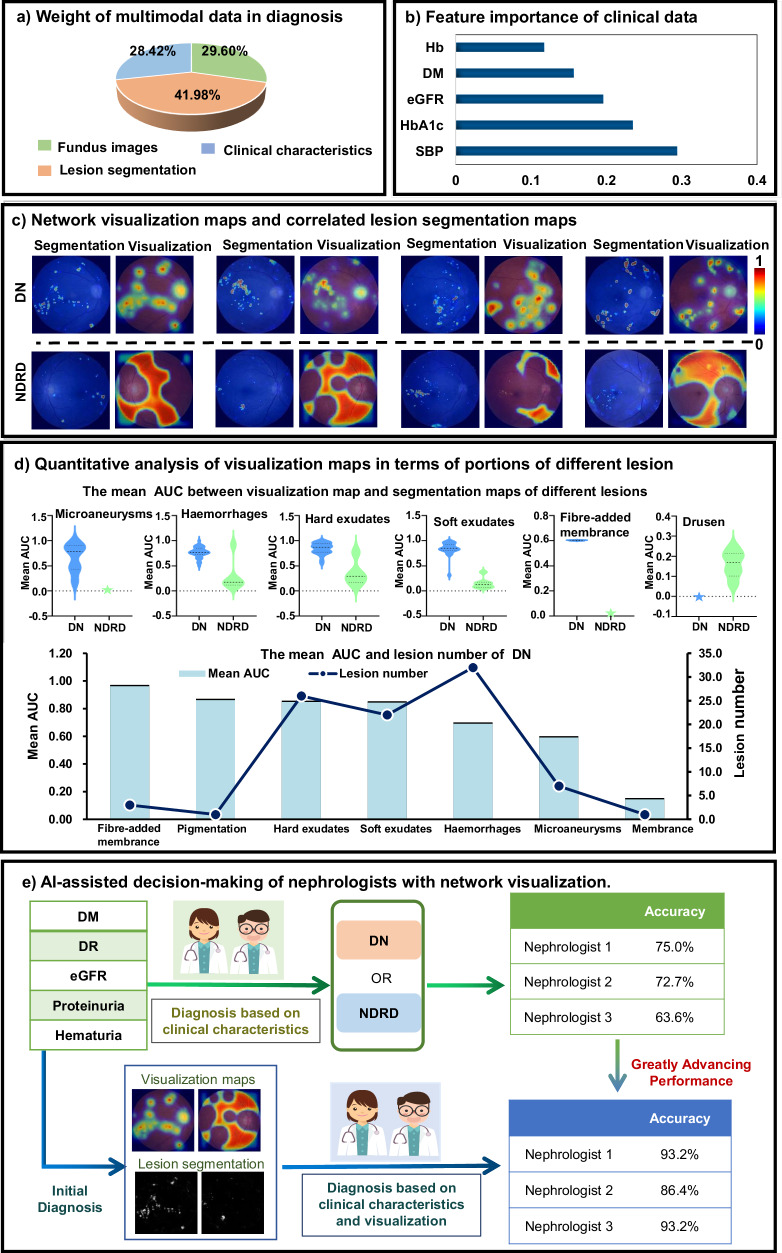
Differentiating between diabetic nephropathy (DN) and non-diabetic renal disease (NDRD) without a kidney biopsy remains a major challenge, often leading to missed opportunities for targeted treatments that could greatly improve NDRD outcomes. To reform the traditional biopsy-all diagnostic paradigm and avoid unnecessary biopsy, we developed a transformer-based deep learning (DL) system for detecting DN and NDRD upon non-invasive multi-modal data of fundus images and clinical characteristics. Our Trans-MUF achieved an AUC of 0.980 (95% CI: 0.979 to 0.980) over the internal retrospective set and also had superior generalizability over a prospective dataset (AUC: 0.989, 95% CI: 0.987 to 0.990) and a multicenter, cross-machine and multi-operator dataset (AUC: 0.932, 95% CI: 0.931 to 0.939). Moreover, the nephrologists' diagnosis accuracy can be improved by 21%, through visualization assistance of the DL system. This paper lays a foundation for automatically differentiating DN and NDRD without biopsy. (Registry name: Correlation Study Between Clinical Phenotype and Pathology of Type 2 Diabetic Nephropathy. ID: NCT03865914. Date: 2017-11-30).
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures



References
-
- Thomas, M. C., Weekes, A. J., Broadley, O. J., Cooper, M. E. & Mathew, T. H. The burden of chronic kidney disease in australian patients with type 2 diabetes (thenefron study). Med. J. Aust.185, 140–144 (2006). - PubMed
-
- Iwai, T. et al. Diabetes mellitus as a cause or comorbidity of chronic kidney disease and its outcomes: the gonryo study. Clin. Exp. Nephrol.22, 328–336 (2018). - PubMed
-
- Anders, H.-J., Davis, J. M. & Thurau, K. Nephron protection in diabetic kidney disease. N. Engl. J. Med.375, 2096–2098 (2016). - PubMed
Associated data
Grants and funding
- L223021/Natural Science Foundation of Beijing Municipality (Beijing Natural Science Foundation)
- 7244305/Natural Science Foundation of Beijing Municipality (Beijing Natural Science Foundation)
- L223021/Natural Science Foundation of Beijing Municipality (Beijing Natural Science Foundation)
- 62250001, 62231002/National Natural Science Foundation of China (National Science Foundation of China)
LinkOut - more resources
Full Text Sources
Medical
