

A meta-analysis of randomized controlled trials: evaluating the efficacy of isokinetic muscle strengthening training in improving knee osteoarthritis outcomes
- PMID: 39856723
- PMCID: PMC11762536
- DOI: 10.1186/s13018-025-05495-8
A meta-analysis of randomized controlled trials: evaluating the efficacy of isokinetic muscle strengthening training in improving knee osteoarthritis outcomes
Abstract
Background: Knee osteoarthritis (KOA) is a prevalent degenerative joint disease. The primary pathological manifestations of KOA include articular cartilage degeneration, joint space narrowing, and osteophyte formation, leading to a spectrum of symptoms, including joint pain, stiffness, reduced mobility, diminished muscle strength, and severe disability. We aimed to utilize a meta-analysis to evaluate the efficacy of isokinetic muscle strengthening training (IMST) as a rehabilitation treatment for KOA in lowland areas.
Methods: The study conducted a comprehensive search of the CNKI, WanFang Data, VIP Database, PubMed, Ovid MEDLINE (1946-), Cochrane Library, Embase, and CBM databases. The databases were conducted from establishing each database to September 31, 2024. The studies included were randomized controlled trials (RCTs) with participants from the plains who met the diagnostic criteria for KOA as outlined in the 2019 edition, with no restrictions on gender, age, or disease course, and no patients with advanced disease; studies where in the control group was either a non-intervention group or a group receiving treatment, other than IMST, and the experimental group received IMST alone or in addition to the treatment administered to the control group; and studies with at least two of the following outcome indicators: (i) knee flexors (Flex)/extensors (Ext) peak torque (PT), (ii) knee Flex/Ext total work (TW), (iii) knee Flex/Ext max rep total work (MRTW), (iv) knee Flex/Ext average power (AP), (v) visual analogue scale (VAS) for pain, (vi) Lequesne index (LI), (vii) Western Ontario and McMaster University Osteoarthritis Index (WOMAC), (viii) Lysholm Knee Scoring Scale (LKSS), (ix) range of motion (ROM) of the knee joint, and (x) 6-min walk test. We systematically reviewed the RCTs in both Chinese and English and evaluated the quality of the included literature. Data were processed and analyzed using ROB 2, RevMan 5.4, Stata17, and GRADEpro. The study protocol was registered on PROSPERO (CRD42024607528).
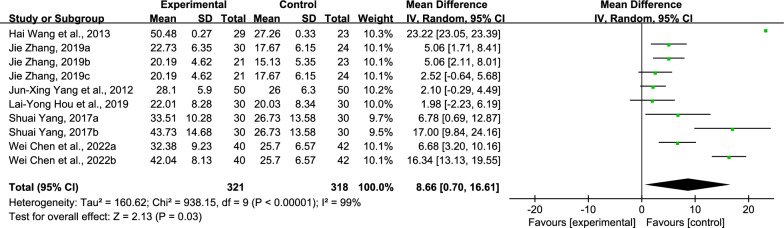
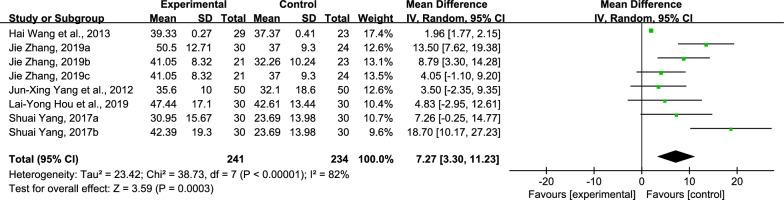
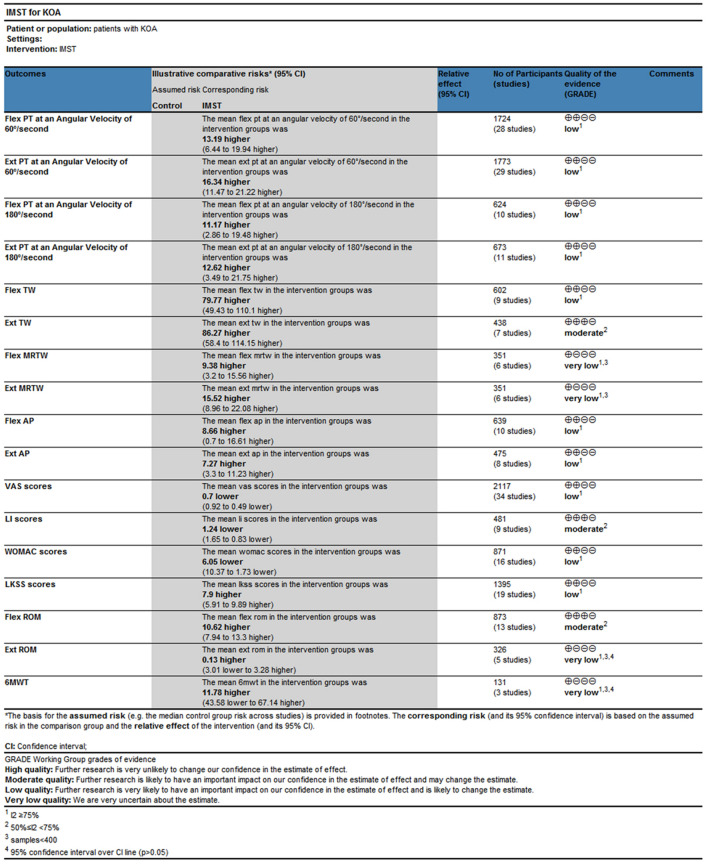
Results: Thirty-three (46 studies, 2,860 patients) had low-to-some concerns risk. IMST significantly improved physical therapy outcomes, including knee Flex PT and knee Ext PT at an angular velocity of 60°/second (standardized mean difference 13.19 [95% confidence interval 6.44, 19.94], P = 0.0001 and 16.34 [11.47, 21.22], P < 0.00001, respectively), and 180°/second (11.17 [2.86, 19.48], P = 0.008 and 12.62 [3.49, 21.75], P = 0.0077, respectively); knee Flex TW (79.77 [49.43, 110.10], P < 0.0001), Ext TW (86.27 [58.40, 114.15], P < 0.00001), knee Flex MRTW (9.38 [3.20, 15.56], P = 0.003), knee Ext MRTW (15.52 [8.96, 22.08], P < 0.0001), knee Flex AP (8.66 [0.70, 16.61], P = 0.03), knee Ext AP (7.27 [3.30, 11.23], P = 0.0003), knee Flex ROM (10.62 [7.94, 13.30], P < 0.00001), and LKSS scores (7.90 [5.91, 9.89], P < 0.00001). Additionally, it reduced VAS scores (- 0.70 [- 0.92, - 0.49], P < 0.00001), LI scores (- 1.24 [- 1.65, - 0.83], P < 0.00001), and WOMAC scores (- 6.05 [- 10.37, - 1.73], P = 0.006). Compared to the control group, superior clinical efficacy was noted in the experimental group. The quality of evidence the studies reported was poor, mainly due to original trials with high inter-study heterogeneity and imprecise results. The therapeutic effect of IMST on KOA remained significant after rigorous testing of subgroup and sensitivity analyses.
Conclusions: In patients with KOA, IMST improves muscle strength and relieves joint pain and stiffness. However, large-scale, high-quality, randomized controlled trials with extended observation periods are urgently needed to popularize the use of IMST in KOA patients.
Keywords: Flexors and extensors; Isokinetic muscle strengthening training; Knee osteoarthritis; Muscle strength; Qinghai-Tibetan plateau.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study is a systematic review. The Research Ethics Committee of Tibet University has confirmed that no ethical approval is required. Informed Consent was obtained from all individual participants included in the study. Consent for publication: No applicable. Competing interests: The authors declare no competing interests.
Figures



















Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Effects of whole-body vibration training as an adjunct to conventional rehabilitation exercise on pain, physical function and disability in knee osteoarthritis: A systematic review and meta-analysis.PLoS One. 2025 Feb 10;20(2):e0318635. doi: 10.1371/journal.pone.0318635. eCollection 2025. PLoS One. 2025. PMID: 39928683 Free PMC article.
-
The Efficacy and Safety of Chinese Herbal Medicine in the Treatment of Knee Osteoarthritis: An Updated Systematic Review and Meta-Analysis of 56 Randomized Controlled Trials.Oxid Med Cell Longev. 2022 Jan 7;2022:6887988. doi: 10.1155/2022/6887988. eCollection 2022. Oxid Med Cell Longev. 2022. PMID: 35035664 Free PMC article.
-
The Effectiveness and Safety of Moxibustion for Treating Knee Osteoarthritis: A PRISMA Compliant Systematic Review and Meta-Analysis of Randomized Controlled Trials.Pain Res Manag. 2019 Dec 17;2019:2653792. doi: 10.1155/2019/2653792. eCollection 2019. Pain Res Manag. 2019. PMID: 31949547 Free PMC article.
-
Quadriceps combined with hip abductor strengthening versus quadriceps strengthening in treating knee osteoarthritis: a study protocol for a randomized controlled trial.BMC Musculoskelet Disord. 2018 May 15;19(1):147. doi: 10.1186/s12891-018-2041-7. BMC Musculoskelet Disord. 2018. PMID: 29764409 Free PMC article. Clinical Trial.
Cited by
-
Effectiveness of exercise therapy in patients with knee osteoarthritis: an overview of systematic reviews.BMJ Open. 2025 Jul 16;15(7):e093163. doi: 10.1136/bmjopen-2024-093163. BMJ Open. 2025. PMID: 40669904 Free PMC article.
-
The Reliability and Validity of an Isometric Knee Strength Measurement Device in Older Adult Individuals.Sensors (Basel). 2025 May 8;25(10):2981. doi: 10.3390/s25102981. Sensors (Basel). 2025. PMID: 40431776 Free PMC article.
References
-
- Chen WH, Liu XX, Tong PJ, Zhan HS, Orthopaedic Professional Committee, Chinese Association of Research and Advancement of Chinese Traditional Medicine, China, Joint Professional Committee, Branch of Orthopaedic of Chinese Association of Integrative Medicine, China. Diagnosis and management of knee osteoarthritis: Chinese medicine expert consensus. Chin J Integr Med. 2016;22:150–3. - PubMed
-
- Sun Q, Zhang KW, Chen JY, Xu Y, Liu Y, Zheng R. Traditional Chinese medicine classification of knee osteoarthritis with proteomics analysis. Ann Palliat Med. 2020;9:3750–6. - PubMed
-
- Yang S. The clinical efficacy of electroacupuncture combined with isometric Concentric training in the treatment of osteoarthritis of knee joints. Beijing University of Chinese Medicine; 2017.
-
- Liao JA, Yeh YC, Chang ZY. The efficacy and safety of traditional Chinese medicine Guilu Erxian Jiao in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Complement Ther Clin Pract. 2022;46: 101515. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
