

Anal Cancer Screening: 10-Year Experience of a Specialized Outpatient Clinic
- PMID: 39857975
- PMCID: PMC11763781
- DOI: 10.3390/cancers17020193
Anal Cancer Screening: 10-Year Experience of a Specialized Outpatient Clinic
Abstract
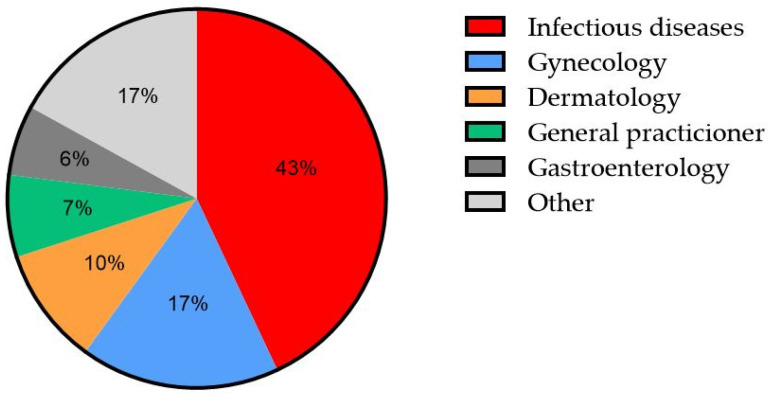
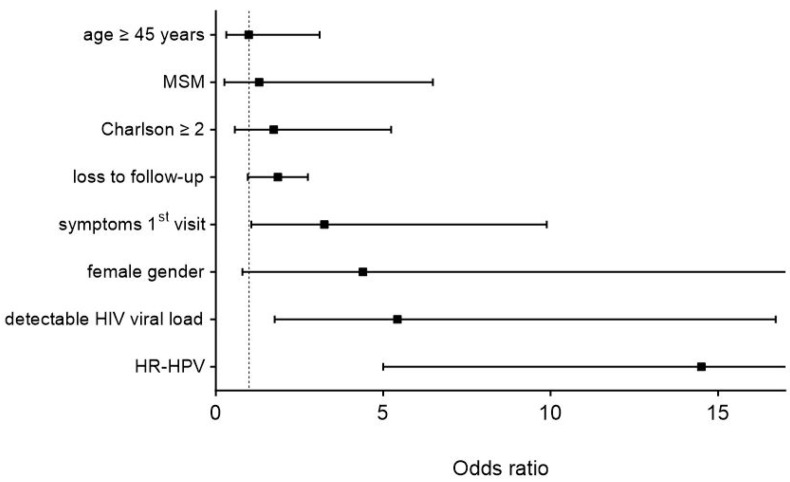
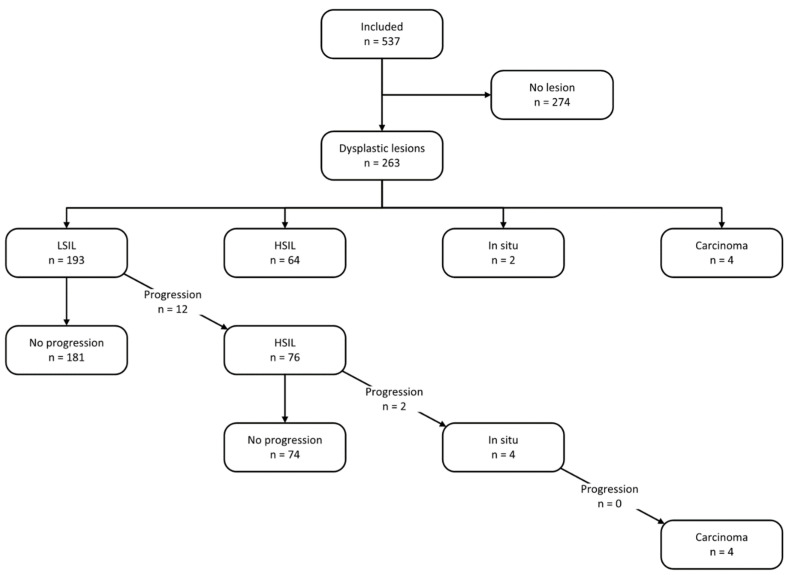
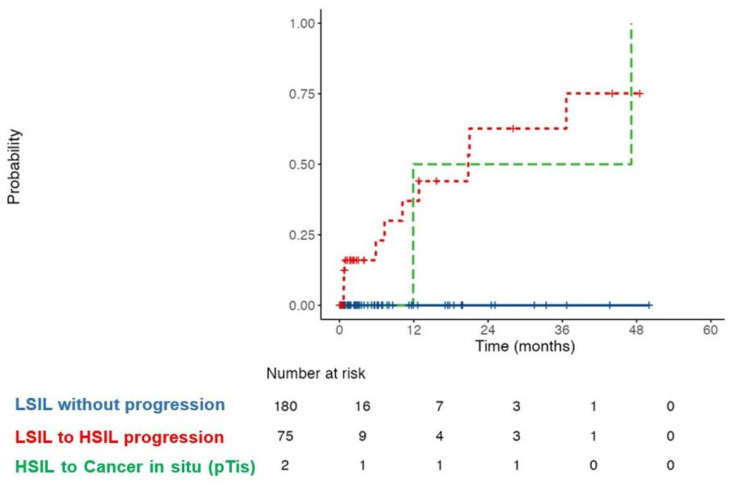
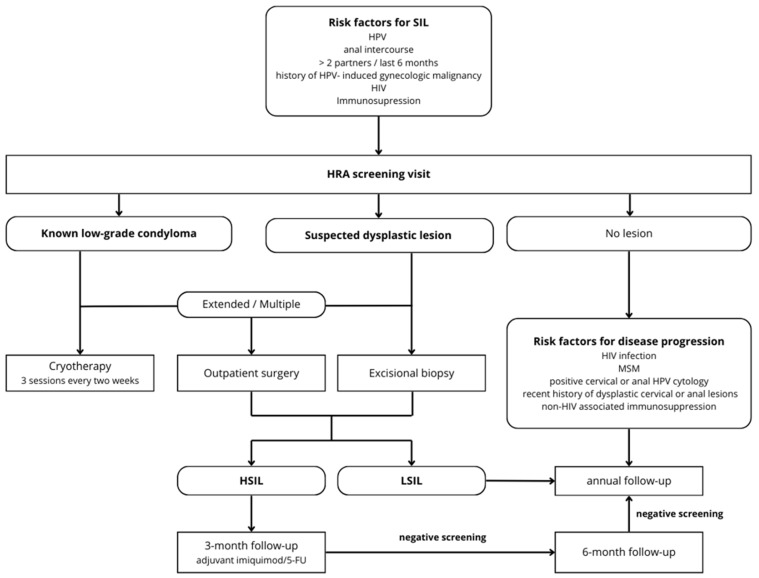
In 2012, the Department of Visceral Surgery of the Lausanne University Hospital CHUV implemented a dedicated high-resolution anoscopy (HRA) outpatient clinic for surveillance and follow-up purposes. This 10-year longitudinal study analyzed 537 patients (2214 visits) using a structured screening protocol. Dysplastic lesions were detected in 49% of patients, predominantly low-grade squamous intraepithelial lesions (LSILs, 74%). Among LSIL cases, 6% progressed to high-grade squamous intraepithelial lesions (HSILs) within 24 months, reaching 25% cumulative progression at 36 months. Of HSIL patients, 3% developed carcinoma in situ after 48 months. Notably, no invasive carcinoma was observed during the follow-up. Four patients diagnosed with squamous cell carcinoma at initial screening were treated with chemoradiotherapy, and one required salvage surgery. Independent risk factors for the presence of higher-stage precancerous lesions (≥HSILs) were the presence of high-risk HPV genotypes (OR 14.5, 95% CI 5-42.2, p < 0.001), detectable HIV viral load (OR 5.4, 95% CI 1.8-16.7, p = 0.003), and symptoms at the first screening visit (OR 3.2, 95% CI 1.1-9.9, p = 0.04). HIV-positive status was associated with a trend towards an increased risk of progression (OR 2.79, p = 0.073). These findings highlight the importance of systematic follow-up and early intervention in high-risk populations to prevent anal cancer progression.
Keywords: HIV; HPV testing; MSM; algorithm; anal cancer; anal dysplasia; high-resolution anoscopy; screening.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Anal Squamous Intraepithelial Lesions (SILs) in Human Immunodeficiency Virus-Positive Men Who Have Sex With Men: Incidence and Risk Factors of SIL and of Progression and Clearance of Low-Grade SILs.J Infect Dis. 2020 Jun 16;222(1):62-73. doi: 10.1093/infdis/jiz614. J Infect Dis. 2020. PMID: 31755920
-
High-resolution anoscopy screening of HIV-positive MSM: longitudinal results from a pilot study.AIDS. 2014 Mar 27;28(6):861-7. doi: 10.1097/QAD.0000000000000160. AIDS. 2014. PMID: 24441516
-
Progression of anal high-grade squamous intraepithelial lesions to invasive anal cancer among HIV-infected men who have sex with men.Int J Cancer. 2014 Mar 1;134(5):1147-55. doi: 10.1002/ijc.28431. Epub 2013 Sep 14. Int J Cancer. 2014. PMID: 23934991
-
The importance of anal cancer screening and high-resolution anoscopy to gastroenterology practice.Curr Opin Gastroenterol. 2020 Sep;36(5):393-401. doi: 10.1097/MOG.0000000000000661. Curr Opin Gastroenterol. 2020. PMID: 32701604 Review.
-
Prognosis and recurrence risk for patients with cervical squamous intraepithelial lesions diagnosed during pregnancy.Cancer. 2004 Aug 25;102(4):228-32. doi: 10.1002/cncr.20428. Cancer. 2004. PMID: 15368314 Review.
Cited by
-
A Brief Review of Anal Cancer Screening Methods for Prevention and Earlier Diagnosis.Cureus. 2025 Mar 16;17(3):e80686. doi: 10.7759/cureus.80686. eCollection 2025 Mar. Cureus. 2025. PMID: 40242694 Free PMC article. Review.
References
-
- Deshmukh A.A., Suk R., Shiels M.S., Damgacioglu H., Lin Y.Y., Stier E.A., Nyitray A.G., Chiao E.Y., Nemutlu G.S., Chhatwal J., et al. Incidence Trends and Burden of Human Papillomavirus-Associated Cancers Among Women in the United States, 2001–2017. J. Natl. Cancer Inst. 2021;113:792–796. doi: 10.1093/jnci/djaa128. - DOI - PMC - PubMed
-
- Sung H., Jiang C., Bandi P., Minihan A., Fidler-Benaoudia M., Islami F., Siegel R.L., Jemal A. Differences in cancer rates among adults born between 1920 and 1990 in the USA: An analysis of population-based cancer registry data. Lancet Public Health. 2024;9:e583–e593. doi: 10.1016/S2468-2667(24)00156-7. - DOI - PubMed
LinkOut - more resources
Full Text Sources
