

Background and Clinical Features of a Unique and Mysterious Autoinflammatory Disease, Schnitzler Syndrome
- PMID: 39859314
- PMCID: PMC11765222
- DOI: 10.3390/ijms26020598
Background and Clinical Features of a Unique and Mysterious Autoinflammatory Disease, Schnitzler Syndrome
Abstract
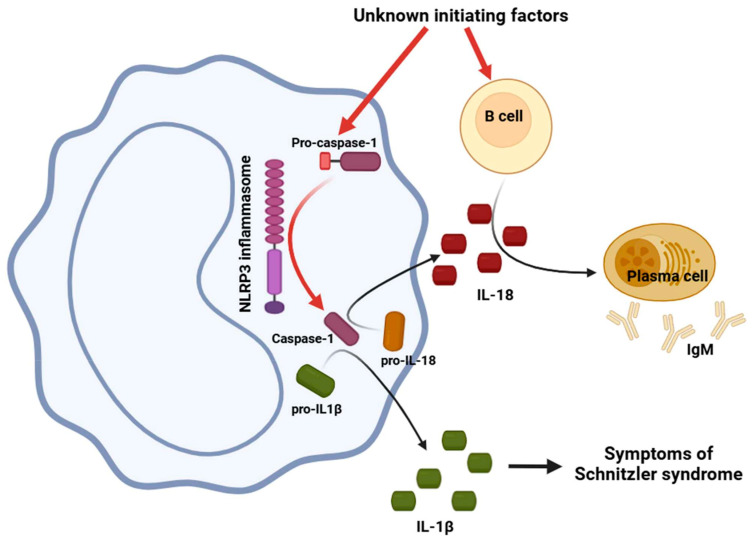
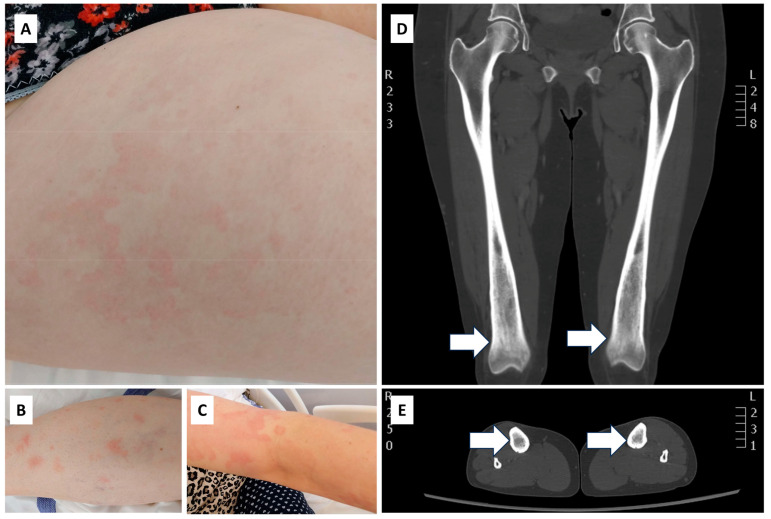
Schnitzler syndrome is a unique autoinflammatory disease, of which 747 cases have been described worldwide to date. The main features of the syndrome are a triad of recurrent urticaria, monoclonal IgM gammopathy, systemic inflammation associated with recurrent fever, joint and bone pain, and atypical bone remodeling (osteosclerosis). The abnormal activation of the NLRP3 inflammasome produces IL-1, which drives the disease pathology, but it also involves IL-6 and IL-18. Unlike other autoinflammatory diseases, Schnitzler syndrome lacks evidence of the gene divergence causing the abnormal activation of NLRP3. However, mutations in the MEFV and MYD88 genes can be associated with the development of the disease. Due to its rarity, diagnosing the disease can be a challenging task. IL-1 inhibitors (i.e., anakinra, canakinumab, and rilonacept) are prominent in the treatment of the disease, but the IL-6 receptor inhibitor tocilizumab and the Bruton's tyrosine kinase inhibitor ibrutinib are also promising alternatives. In this summary article, we aim to provide a comprehensive overview of the clinical and molecular background of the disease and potential therapeutic targets, based on the cases reported so far. We diagnosed a patient who, to the best of our knowledge, represents the 748th documented case of this specific pathology. In the context of this patient, we would also like to draw attention to the potential pathogenic role of two novel gene mutations (variants of the MEFV gene "c.2084A>G" and the F2 gene "3'UTR c.*97G>A").
Keywords: F2 gene; MEFV gene; Schnitzler syndrome; anakinra; autoinflammatory disease; canakinumab; diagnosis; monoclonal IgM; urticaria.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Molecular genetic investigation, clinical features, and response to treatment in 21 patients with Schnitzler syndrome.Blood. 2018 Mar 1;131(9):974-981. doi: 10.1182/blood-2017-10-810366. Epub 2017 Dec 28. Blood. 2018. PMID: 29284595 Free PMC article. Clinical Trial.
-
Schnitzler syndrome and Schnitzler-like syndromes.Chin Med J (Engl). 2022 May 20;135(10):1190-1202. doi: 10.1097/CM9.0000000000002015. Chin Med J (Engl). 2022. PMID: 35089885 Free PMC article.
-
Refractory serum immunoglobulin M elevation during anti-interleukin (IL)-1- or IL-6-targeted treatment in four patients with Schnitzler syndrome.J Dermatol. 2021 Nov;48(11):1789-1792. doi: 10.1111/1346-8138.16124. Epub 2021 Aug 26. J Dermatol. 2021. PMID: 34435697
-
[Schnitzler syndrome: diagnostics and treatment].Klin Onkol. 2011;24(4):271-7. Klin Onkol. 2011. PMID: 21905617 Review. Czech.
-
Similarities and differences in autoinflammatory diseases with urticarial rash, cryopyrin-associated periodic syndrome and Schnitzler syndrome.Allergol Int. 2023 Jul;72(3):385-393. doi: 10.1016/j.alit.2023.02.005. Epub 2023 Mar 10. Allergol Int. 2023. PMID: 36906447 Review.
References
-
- Bibas M., Sarosiek S., Castillo J.J. Waldenström Macroglobulinemia—A State-of-the-Art Review: Part 1: Epidemiology, Pathogenesis, Clinicopathologic Characteristics, Differential Diagnosis, Risk Stratification, and Clinical Problems. Mediterr. J. Hematol. Infect. Dis. 2024;16:e2024061. doi: 10.4084/MJHID.2024.061. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
