

Combined Multilayered Amniotic Membrane Graft and Fibrin Glue as a Surgical Management of Limbal Dermoid Cyst
- PMID: 39860612
- PMCID: PMC11765613
- DOI: 10.3390/jcm14020607
Combined Multilayered Amniotic Membrane Graft and Fibrin Glue as a Surgical Management of Limbal Dermoid Cyst
Abstract
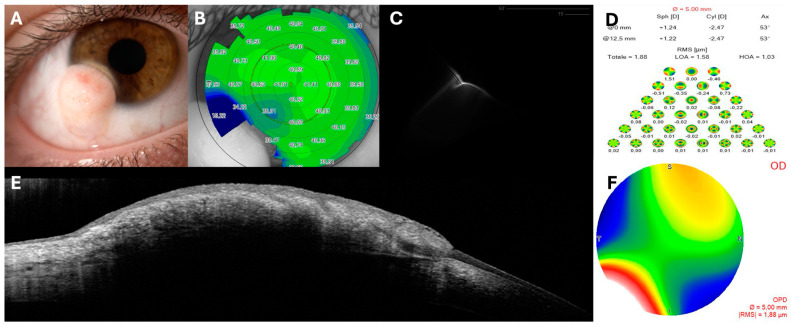
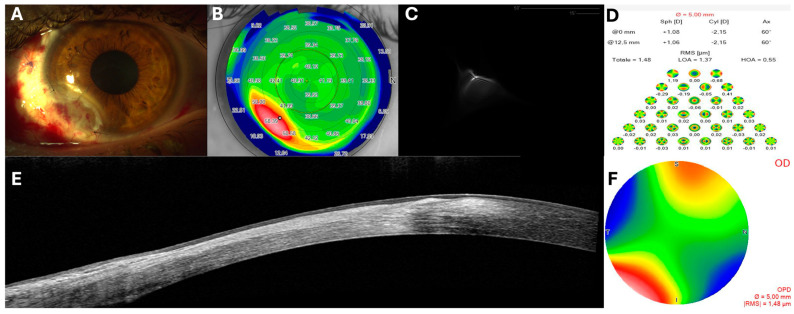
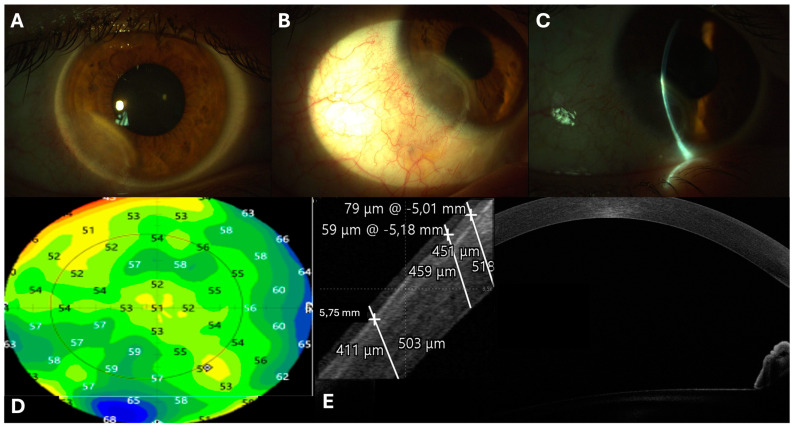
Background/Objectives: To report the cosmetic, clinical, and visual outcomes of a combined surgical approach for treating a corneal/limbal dermoid using excision and a three-layered amniotic membrane graft with fibrin glue. Methods: An 18-year-old female presented with impaired vision and ocular discomfort caused by a prominent dome-shaped limbal congenital dermoid on the inferotemporal cornea, resulting in a significant aesthetic concern. A full assessment, including refraction, best-corrected visual acuity (BCVA), corneal topography, aberrometry and anterior segment OCT (AS-OCT) was conducted to plan the surgical approach. The dermoid was excised under peribulbar anaesthesia using manual lamellar dissection, followed by the application of 0.02% Mitomycin C and a multilayered amniotic membrane graft with fibrin glue. A bandage contact lens was applied and removed after three weeks, with postoperative treatment including topical antibiotics and steroids. Follow-ups were conducted on day 1, at 1 week, 3 weeks, 2 months, 6 months, 1 year, and 2 years. Results: Histopathological examination confirmed the mesoblastic nature of the lesion. Significant improvements in BCVA and ocular symptoms were observed. Corneal topography showed ocular surface regularization with reduction of high order aberrations and point spread function. AS-OCT showed complete integration of the amniotic membrane, with full epithelial coverage of the defect. The healing process was uneventful and the ocular surface remained stable throughout the entire follow-up, without complications or recurrence. Conclusions: This approach of dermoid excision, multilayered amniotic membrane and fibrin glue restored vision effectively, with notable improvements in ocular surface and cosmetic outcomes, without recurrence over two years.
Keywords: amniotic membrane; corneal dermoid; fibrin glue; mitomycin C.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Progressive large pediatric corneal limbal dermoid management with tissue glue-assisted monolayer amniotic membrane transplantation: A case report.Medicine (Baltimore). 2018 Nov;97(46):e13084. doi: 10.1097/MD.0000000000013084. Medicine (Baltimore). 2018. PMID: 30431578 Free PMC article.
-
Combined superficial keratectomy, alcohol delamination and amniotic membrane patch with fibrin glue in Salzmann nodular degeneration.Eur J Ophthalmol. 2024 Jul;34(4):1281-1285. doi: 10.1177/11206721241251890. Epub 2024 Apr 26. Eur J Ophthalmol. 2024. PMID: 38676318
-
Limbal stem cell transplantation: an evidence-based analysis.Ont Health Technol Assess Ser. 2008;8(7):1-58. Epub 2008 Oct 1. Ont Health Technol Assess Ser. 2008. PMID: 23074512 Free PMC article.
-
Lamellar keratoplasty using femtosecond laser intrastromal lenticule for limbal dermoid: case report and literature review.J Int Med Res. 2018 Nov;46(11):4753-4759. doi: 10.1177/0300060518790874. Epub 2018 Aug 8. J Int Med Res. 2018. PMID: 30088427 Free PMC article. Review.
-
[Simple limbal epithelial transplantation (SLET) : A simple technique for the treatment of unilateral complete limbal stem cell deficiency. Video article].Ophthalmologe. 2021 Apr;118(4):404-412. doi: 10.1007/s00347-021-01346-z. Epub 2021 Mar 8. Ophthalmologe. 2021. PMID: 33683425 Review. German.
Cited by
-
Novel Surgical Approach for Limbal Dermoid Excision: Utilizing Bowman's Membrane Lenticule and Autologous Limbal Stem Cell Transplantation for Enhanced Epithelial Healing and Visual Outcomes.Vision (Basel). 2025 Jul 11;9(3):56. doi: 10.3390/vision9030056. Vision (Basel). 2025. PMID: 40700084 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
