

Vitamin D: Evidence-Based Health Benefits and Recommendations for Population Guidelines
- PMID: 39861407
- PMCID: PMC11767646
- DOI: 10.3390/nu17020277
Vitamin D: Evidence-Based Health Benefits and Recommendations for Population Guidelines
Abstract
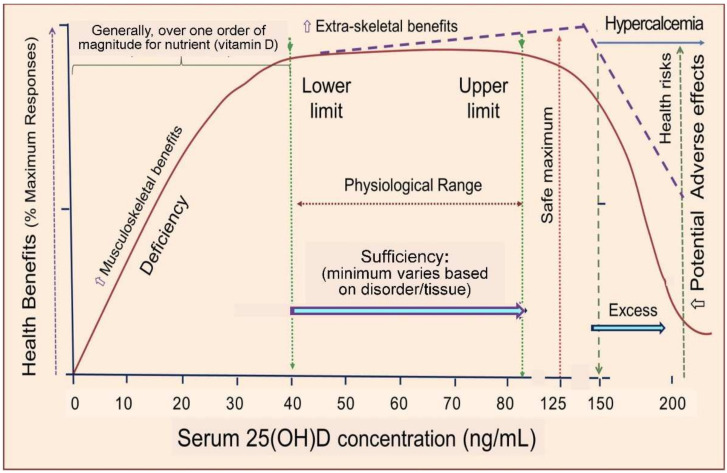
Vitamin D offers numerous under-recognized health benefits beyond its well-known role in musculoskeletal health. It is vital for extra-renal tissues, prenatal health, brain function, immunity, pregnancy, cancer prevention, and cardiovascular health. Existing guidelines issued by governmental and health organizations are bone-centric and largely overlook the abovementioned extra-skeletal benefits and optimal thresholds for vitamin D. In addition, they rely on randomized controlled trials (RCTs), which seldom show benefits due to high baseline 25-hydroxyvitamin D [25(OH)D] concentrations, moderate supplementation doses, and flawed study designs. This review emphasizes the findings from prospective cohort studies showing that higher 25(OH)D concentrations reduce the risks of major diseases and mortality, including pregnancy and birth outcomes. Serum concentrations > 30 ng/mL (75 nmol/L) significantly lower disease and mortality risks compared to <20 ng/mL. With 25% of the U.S. population and 60% of Central Europeans having levels <20 ng/mL, concentrations should be raised above 30 ng/mL. This is achievable through daily supplementation with 2000 IU/day (50 mcg/day) of vitamin D3, which prevent diseases and deaths. Furthermore, a daily dose between 4000 and 6000 IU of vitamin D3 to achieve serum 25(OH)D levels between 40 and 70 ng/mL would provide greater protection against many adverse health outcomes. Future guidelines and recommendations should integrate the findings from observational prospective cohort studies and well-designed RCTs to improve public health and personalized care.
Keywords: COVID-19; Endocrine Society; cancer; cardiovascular disease; chronic kidney disease; chronic lower respiratory diseases; dementia; diabetes mellitus; pregnancy.
Conflict of interest statement
W.B.G. received grants for vitamin D research from Bio-Tech Pharmacal, Inc. (Fayetteville, AR, USA) for many years until the end of 2023. The other authors declare no conflicts of interest.
Figures


References
-
- Demay M.B., Pittas A.G., Bikle D.D., Diab D.L., Kiely M.E., Lazaretti-Castro M., Lips P., Mitchell D.M., Murad M.H., Powers S., et al. Vitamin D for the Prevention of Disease: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2024;109:1907–1947. doi: 10.1210/clinem/dgae290. - DOI - PubMed
-
- Holick M.F., Binkley N.C., Bischoff-Ferrari H.A., Gordon C.M., Hanley D.A., Heaney R.P., Murad M.H., Weaver C.M., Endocrine S. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011;96:1911–1930. doi: 10.1210/jc.2011-0385. - DOI - PubMed
-
- Kroll M.H., Bi C., Garber C.C., Kaufman H.W., Liu D., Caston-Balderrama A., Zhang K., Clarke N., Xie M., Reitz R.E., et al. Temporal relationship between vitamin D status and parathyroid hormone in the United States. PLoS ONE. 2015;10:e0118108. doi: 10.1371/journal.pone.0118108. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
