

The vestibular and oculomotor dysfunction in Fabry disease: a cohort study in China
- PMID: 39862133
- PMCID: PMC11770862
- DOI: 10.1080/07853890.2025.2453626
The vestibular and oculomotor dysfunction in Fabry disease: a cohort study in China
Abstract
Objective: Whereas a few studies have evaluated vestibular involvement in Fabry disease (FD), the relationship between vestibular/oculomotor abnormalities and disease-specific biomarkers remain unclear. Therefore, we seek to evaluate these quantitatively and analyze their relationship with disease phenotype and biomarkers in FD.
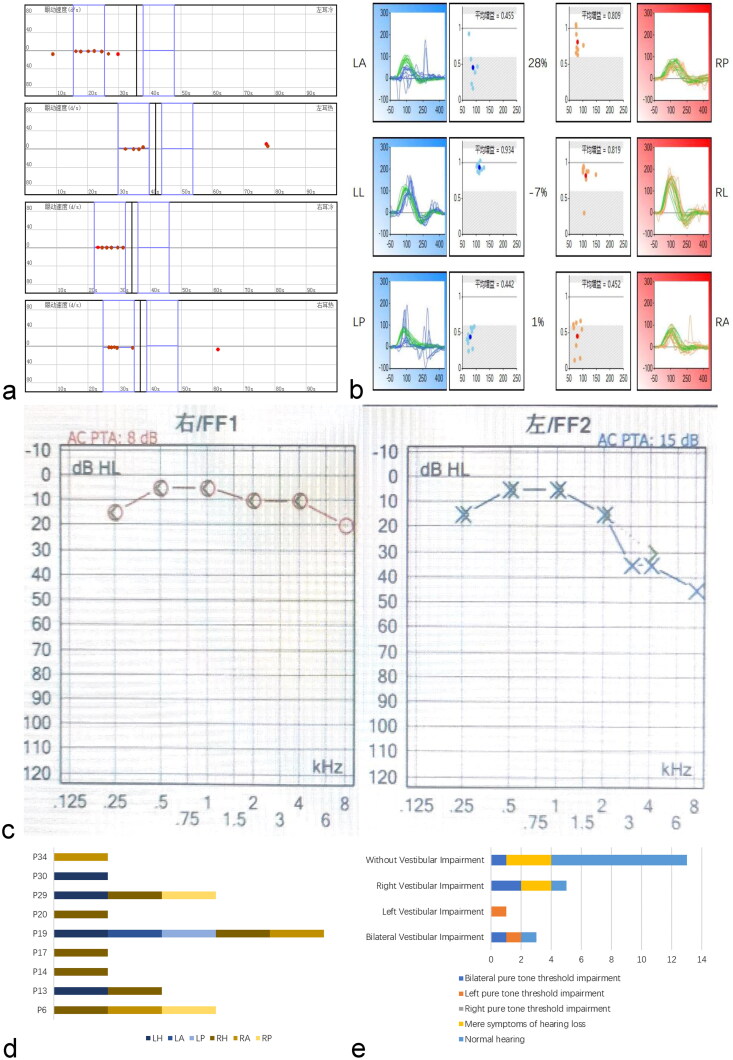
Methods: This cohort study enrolled 37 Chinese FD patients registered in our center. The vestibular/oculomotor examinations were performed, including the videonystagmography, the caloric test and the video head-impulse test. Statistical analyses were made between different subgroups of patients.
Results: Visuo-oculomotor dysfunctions were found in 30/37 (81.1%) patients. Vestibulo-oculomotor dysfunctions were revealed in 9/22 (40.9%) patients. Statistical tests showed: (1) significantly higher Mainz Severity Score Index in patients with prolonged saccade latency [20(18,33) VS 13(9,22), p = 0.008] and vestibulo-oculomotor dysfunction [23(20,31) VS 9(5.5,12.5), p = 0.024], (2) significantly higher total small-vessel disease score in subgroups with prolonged saccade latency [2.5(1,3.5) VS 1(0,2), p = 0.038], defective smooth pursuit [3(2,4) VS 1(0,2), p = 0.003], defective optokinetic nystagmus [4(2,4) VS 1(0.2), p = 0.009] and vestibulo-oculomotor dysfunction [1(1,3) VS 0(0,1), p = 0.028], (3) significantly lower α-Gal A activity (μmol/L/h) in subgroups with defective saccades [0.44(0.25,1.93) VS 1.85(0.75,5.52), p = 0.015] and defective smooth pursuit [0.30(0.17,0.44) VS 0.96(0.39,2.40), p = 0.008], and (4) significantly elevated plasma globotriaosylsphingosine (ng/ml) in patients with defective saccades [74.16(11.05,89.18) VS 10.64(7.08,36.32), p = 0.034], than in patients without those abnormalities.
Conclusion: A high incidence of extensive vestibular and oculomotor dysfunction was observed in patients with FD, with the neuro-otological dysfunction being closely related to the disease burden and biomarkers like α-Gal A activity and lyso-Gb3.
Keywords: Fabry disease; cerebral small vessel disease; eye movement; globotriaosylsphingosine; mainz severity score index; vestibular disorders.
Plain language summary
The extensive vestibular and oculomotor dysfunction in FD patients were closely related to the disease burden and biomarkers like α-Gal A activity and lyso-Gb3.When vestibular dysfunction is identified in FD patients, a multi-system evaluation should be conducted to early discover the damage of important organs.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical