

Colonic strictures in Crohn's disease: a non-surgical survival
- PMID: 39862140
- PMCID: PMC11776860
- DOI: 10.1080/20565623.2025.2455911
Colonic strictures in Crohn's disease: a non-surgical survival
Abstract
Background: Colonic stenosis in Crohn's disease (CD) is uncommon, and data on surgery-free survival are limited. This study aimed to determine surgery-free survival rates and identify associated factors.
Patients and methods: A retrospective study was conducted from 2003 to 2022, including patients with CD complicated by colonic stenosis. Patients with uncertain diagnoses or follow-up periods of less than six months were excluded.
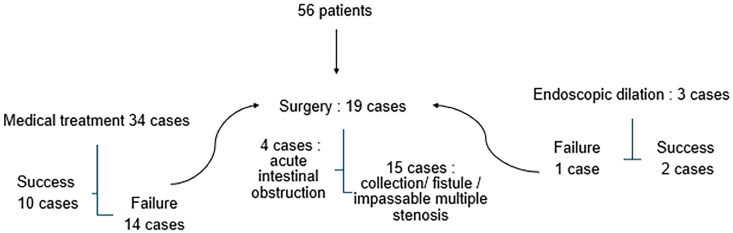
Results: Fifty-six patients were included (median age 44 years [range 14-65], male-to-female ratio = 0.93). Surgery-free survival rates were 58.9% at 6 months, 43.7% at 2 years, and 31.7% at 5 years, with an average surgery-free survival of 46.7 months. Univariate analysis showed that joint manifestations (p = 0.01), corticosteroids (p = 0.02), anti-TNF alpha (p = 0.02), salicylates (p = 0.02), and azathioprine (p = 0.01) increased surgery-free survival. Complications such as collections or internal fistulas (p = 0.03), parietal ulceration on imaging (p = 0.01), and acute intestinal obstruction (p = 0.01) were associated with reduced surgery-free survival. In multivariate analysis, biologic therapy was the only independent protective factor against surgery (p = 0.001, OR = 0.19).
Conclusion: The early introduction of biologic therapy is crucial for increasing surgery-free survival in patients with colonic stenosis in CD, given the limited effectiveness of conventional treatments.
Keywords: Crohn’s disease; Inflammatory bowel disease; anti TNF alpha therapy; colonic stricture; medical treatment; prognostic; surgery; survival.
Plain language summary
Colonic stenosis in CD is rare and lacks standardized management.Data on survival without surgery and associated factors are scarce.Study aims to determine surgery-free survival rates and identify influencing factors.Retrospective study on ileocolonic or colonic CD with colonic stenosis.Inclusion period: January 2003 to December 2022.Exclusions: Uncertain CD, tuberculosis, cancer, dysplasia56 patients included; median age at diagnosis = 44 years; male-to-female ratio = 0.93.Surgery-free survival: 58.9% at 6 months, 43.7% at 2 years, 31.7% at 5 years; average = 46.7 months (3.9 years).Univariate analysis linked joint manifestations, corticosteroids, IFX, ADA, salicylates, AZA to increased surgery-free survival. Complications, parietal ulceration, acute intestinal obstruction associated with reduced surgery-free survival.Multivariate analysis identified anti TNF alpha as the only independent protective factor against surgery (p = 0.001, OR = 0.19).
Conflict of interest statement
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures




References
-
- Rieder F, Fiocchi C, Rogler G.. Mechanisms, management, and treatment of fibrosis in patients with inflammatory bowel diseases. Gastroenterology. 2017;152(2):340–350.e6. doi: 10.1053/j.gastro.2016.09.047 - DOI - PMC - PubMed
-
* (Provides a comprehensive overview of fibrosis mechanisms in inflammatory bowel diseases, essential for understanding the development of stenosis in Crohn’s disease.)
LinkOut - more resources
Full Text Sources
Research Materials