

Influence of frailty status on the incidence of intraoperative hypotensive events in elective surgery: Hypo-Frail, a single-centre retrospective cohort study
- PMID: 39863473
- PMCID: PMC12598938
- DOI: 10.1016/j.bja.2024.10.050
Influence of frailty status on the incidence of intraoperative hypotensive events in elective surgery: Hypo-Frail, a single-centre retrospective cohort study
Abstract
Background: Frailty is a predictor of morbidity and mortality in older patients. This study aimed to investigate the influence of frailty status on likelihood, rate, duration, and severity of intraoperative hypotension (IOH), which can lead to severe organ dysfunction.
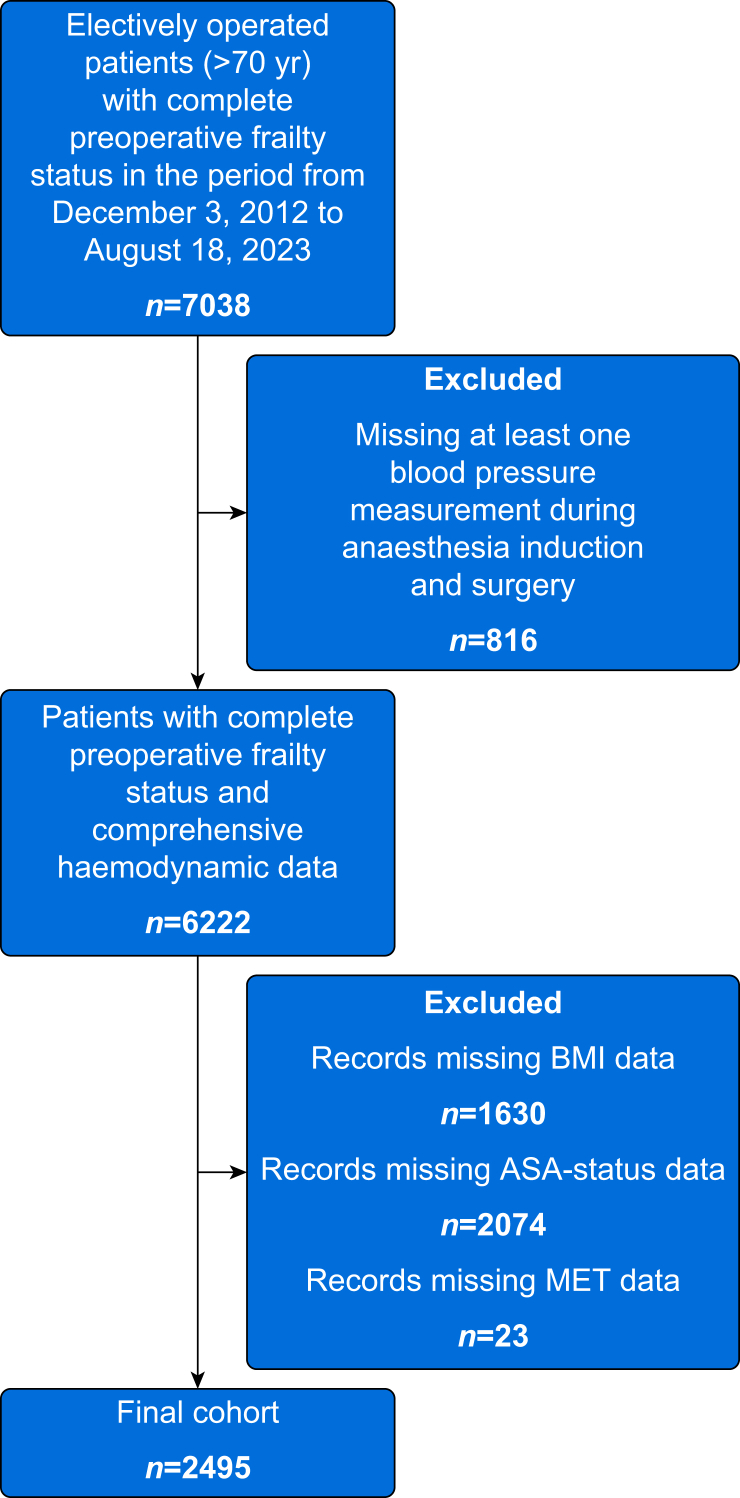
Methods: Surgical patients (≥70 yr old) with preoperative frailty assessment were analysed retrospectively. Frailty status was defined as robust, prefrail, or frail based on modified Fried criteria. IOH was defined as mean arterial pressure <65 mm Hg. For likelihood, rate, duration, and severity of IOH, logistic and Poisson regression were used.
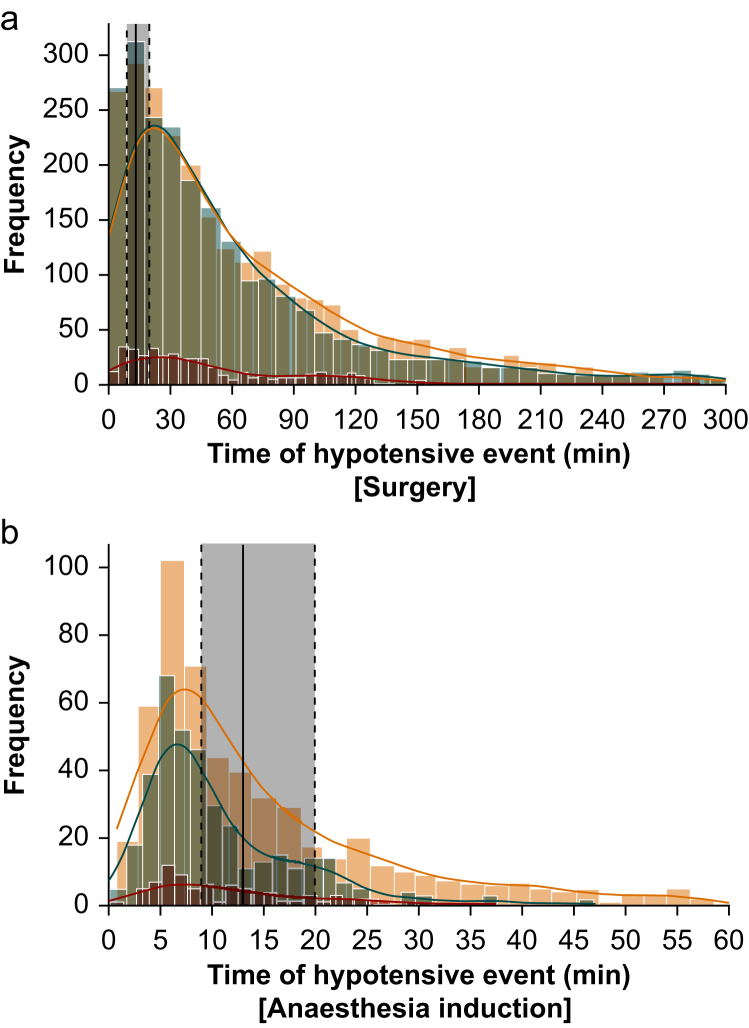
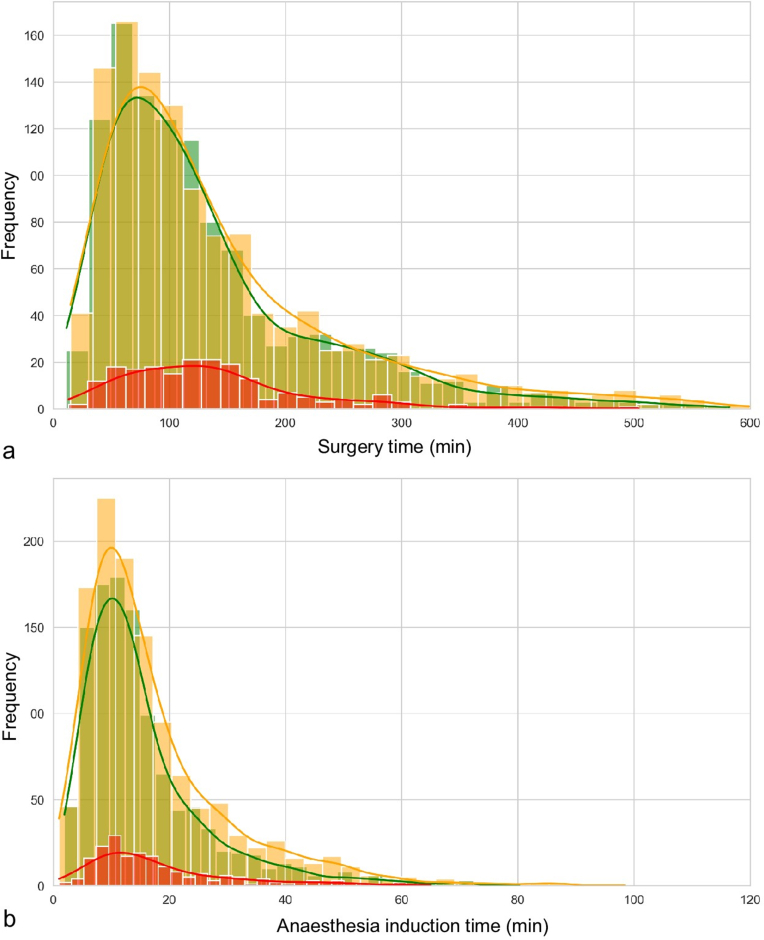
Results: We included 2495 patients. There was no significant difference in likelihood of IOH. An increase of 9% in rate of IOH during surgery for prefrail (incidence rate ratio [IRR] 1.09 [95% CI 1.03-1.16], P=0.002), and 16% increase for frail patients (IRR 1.16 [1.04-1.29], P=0.007) was observed. During anaesthesia induction, prefrail patients exhibited a 28% increase in IOH (IRR 1.28 [1.12-1.47], P<0.001). Although there were no differences in the severity of IOH if surgery or anaesthesia induction duration was taken into account, frailty status was associated with a 15% longer time-weighted duration of IOH during anaesthesia induction (IRR 1.15 [1.06-1.24], P=0.001). Mediator analysis revealed that frailty status accounted for >90% after considering number of measured blood pressures and surgical duration and >70% after accounting for total propofol dose.
Conclusions: Prefrail and frail patients aged ≥70 yr experienced up to 16% more IOH during surgery and 28% more during anaesthesia induction compared with robust patients. Preoperative optimisation (prehabilitation) and modification of intraoperative management (e.g. invasive blood pressure management) have the potential to reduce IOH in prefrail and frail patients.
Keywords: frailty; geriatric anaesthesia; haemodynamics; hypotension; risk assessment.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interest The authors declare that they have no conflicts of interest.
Figures

References
-
- Dasgupta M., Rolfson D.B., Stolee P., Borrie M.J., Speechley M. Frailty is associated with postoperative complications in older adults with medical problems. Arch Gerontol Geriatr. 2009;48:78–83. - PubMed
-
- Makary M.A., Segev D.L., Pronovost P.J., et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210:901–908. - PubMed
-
- Robinson T.N., Eiseman B., Wallace J.I., et al. Redefining geriatric preoperative assessment using frailty, disability and co-morbidity. Ann Surg. 2009;250:449–455. - PubMed
-
- Wesselink E.M., Kappen T.H., Torn H.M., Slooter A.J.C., van Klei W.A. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. Br J Anaesth. 2018;121:706–721. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
