

Development and validation of an EHR-based risk prediction model for geriatric patients undergoing urgent and emergency surgery
- PMID: 39865251
- PMCID: PMC11771050
- DOI: 10.1186/s12871-024-02880-4
Development and validation of an EHR-based risk prediction model for geriatric patients undergoing urgent and emergency surgery
Abstract
Background: Clinical determination of patients at high risk of poor surgical outcomes is complex and may be supported by clinical tools to summarize the patient's own personalized electronic health record (EHR) history and vitals data through predictive risk models. Since prior models were not readily available for EHR-integration, our objective was to develop and validate a risk stratification tool, named the Assessment of Geriatric Emergency Surgery (AGES) score, predicting risk of 30-day major postoperative complications in geriatric patients under consideration for urgent and emergency surgery using pre-surgical existing electronic health record (EHR) data.
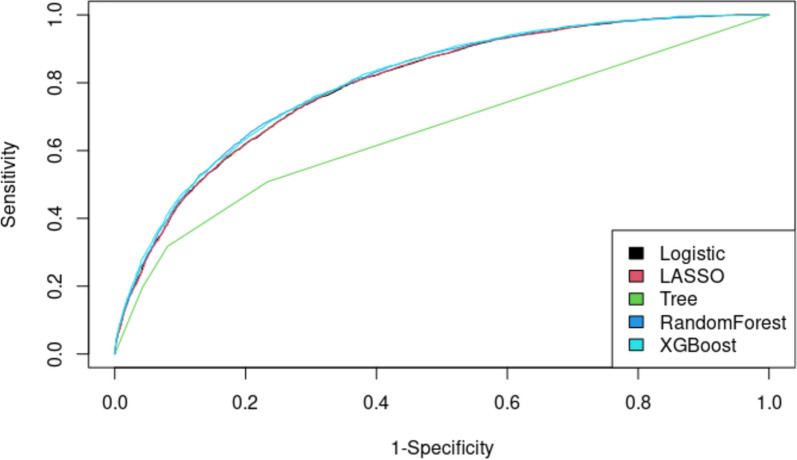
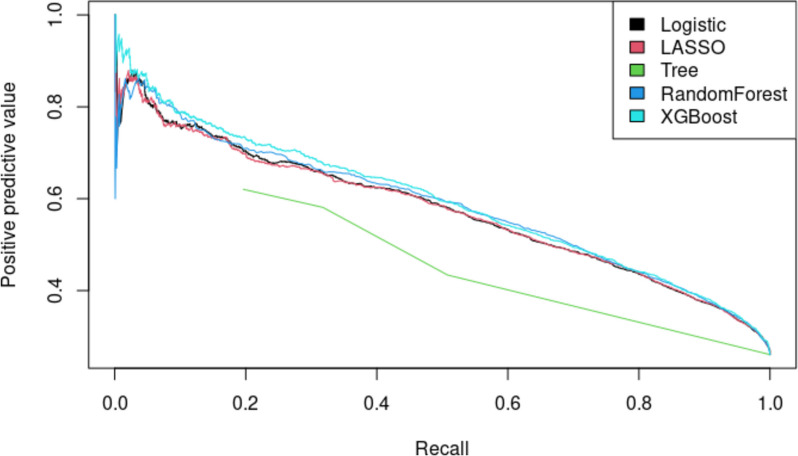
Methods: Patients 65-years and older undergoing urgent or emergency non-cardiac surgery within 21 hospitals 2017-2021 were used to develop the model (randomly split: 80% training, 20% test). The primary outcome was a 30-day composite outcome including several postoperative major complications and mortality; secondary outcomes included common individual complications included in the primary composite outcome (sepsis, progressive renal insufficiency or renal failure, and mortality). Patients' EHR-based clinical history, vital signs, labs, and demographics were included in logistic regression, LASSO, decision tree, Random Forest, and XGBoost models. Area under the receiver operating characteristics curve (AUCROC) was used to compare model performance.
Results: Overall, 66,262 patients (median [IQR] age 78 [(70.9-84.0], female 53.9%, White race 68.5%) received urgent or emergency non-cardiac surgery (25.7% orthopedic cases, 21.9% general surgery cases). AUCROC ranged from 0.655 (Decision Tree) - 0.804 (XGBoost) for the primary composite outcome. XGBoost AUCROC was 0.823, 0.781, and 0.839 in predicting outcomes of sepsis, progressive renal insufficiency or renal failure, and mortality, respectively.
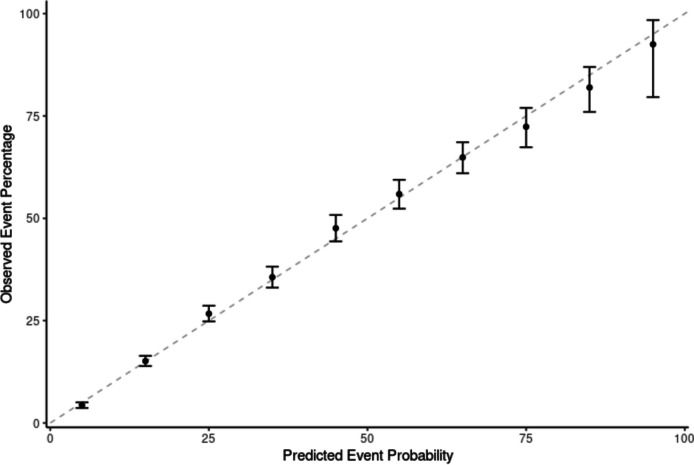
Conclusions: We developed a model to accurately predict major postoperative complications in geriatric patients undergoing urgent or emergency surgery using the patient's own existing EHR data. EHR implementation of this model could efficiently support clinicians' surgical risk assessment and perioperative decision-making discussions in this vulnerable patient population.
Keywords: Emergency surgery; Geriatric surgery; Risk prediction model.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in accordance with the ethical principles of the Belmont Report. This study was approved by the Kaiser Foundation Institute’s Institutional Review Board (1900880–5) and the requirement for written informed consent was waived. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Developing a Machine Learning Model for Predicting 30-Day Major Adverse Cardiac and Cerebrovascular Events in Patients Undergoing Noncardiac Surgery: Retrospective Study.J Med Internet Res. 2025 Apr 9;27:e66366. doi: 10.2196/66366. J Med Internet Res. 2025. PMID: 40203300 Free PMC article.
-
The statistical importance of P-POSSUM scores for predicting mortality after emergency laparotomy in geriatric patients.BMC Med Inform Decis Mak. 2020 May 7;20(1):86. doi: 10.1186/s12911-020-1100-9. BMC Med Inform Decis Mak. 2020. PMID: 32380980 Free PMC article.
-
Development and Validation of a Routine Electronic Health Record-Based Delirium Prediction Model for Surgical Patients Without Dementia: Retrospective Case-Control Study.JMIR Perioper Med. 2025 Jan 9;8:e59422. doi: 10.2196/59422. JMIR Perioper Med. 2025. PMID: 39786865 Free PMC article.
-
What is the utility of preoperative frailty assessment for risk stratification in cardiac surgery?Interact Cardiovasc Thorac Surg. 2013 Aug;17(2):398-402. doi: 10.1093/icvts/ivt197. Epub 2013 May 10. Interact Cardiovasc Thorac Surg. 2013. PMID: 23667068 Free PMC article. Review.
-
Perioperative risk assessment for emergency general surgery in those with multimorbidity or frailty.Curr Opin Crit Care. 2025 Jun 1;31(3):252-261. doi: 10.1097/MCC.0000000000001269. Epub 2025 Mar 19. Curr Opin Crit Care. 2025. PMID: 40156265 Review.
References
-
- Gale SC, Shafi S, Dombrovskiy VY, et al. The public health burden of emergency general surgery in the United States: a 10-year analysis of the Nationwide Inpatient Sample–2001 to 2010. J Trauma Acute Care Surg. 2014;77(2):202–8. 10.1097/TA.0000000000000362. - PubMed
-
- Yap EN, Dusendang JR, Ng KP, et al. Risk of cardiac events after elective versus urgent or emergent noncardiac surgery: Implications for quality measurement and improvement. J Clin Anesth. 2023;84:110994. 10.1016/j.jclinane.2022.110994. - PubMed
-
- McCoy CC, Englum BR, Keenan JE, et al. Impact of specific postoperative complications on the outcomes of emergency general surgery patients. J Trauma Acute Care Surg. 2015;78(5):912–8. 10.1097/TA.0000000000000611. discussion 918-9. - PubMed
-
- Turrentine FE, Wang H, Simpson VB, et al. Surgical risk factors, morbidity, and mortality in elderly patients. J Am Coll Surg. 2006;203(6):865–77. 10.1016/j.jamcollsurg.2006.08.026. - PubMed
-
- Desserud KF, Veen T, Søreide K. Emergency general surgery in the geriatric patient. Br J Surg. 2016;103(2):e52-61. 10.1002/bjs.10044. - PubMed
