

Second-generation anti-amyloid monoclonal antibodies for Alzheimer's disease: current landscape and future perspectives
- PMID: 39865265
- PMCID: PMC11771116
- DOI: 10.1186/s40035-025-00465-w
Second-generation anti-amyloid monoclonal antibodies for Alzheimer's disease: current landscape and future perspectives
Abstract
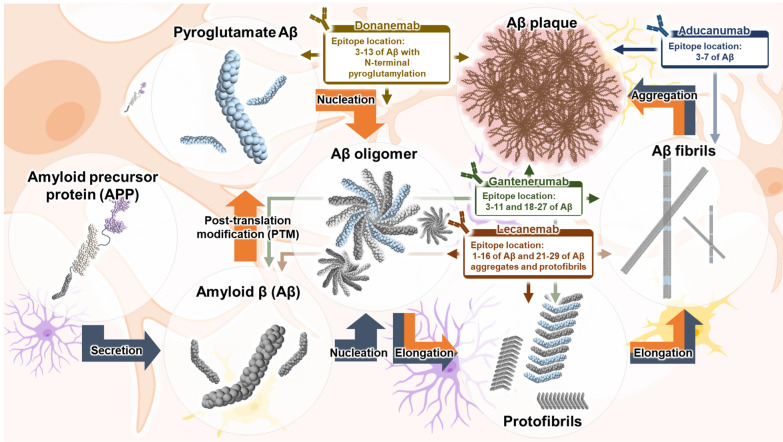
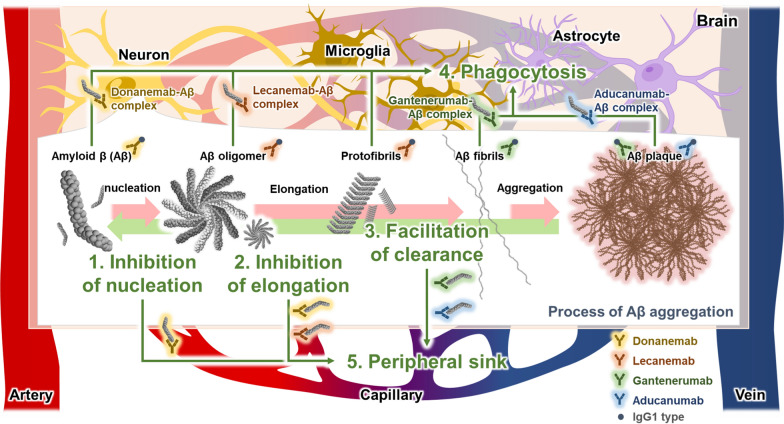
Alzheimer's disease (AD) is the most common type of dementia. Monoclonal antibodies (MABs) serve as a promising therapeutic approach for AD by selectively targeting key pathogenic factors, such as amyloid-β (Aβ) peptide, tau protein, and neuroinflammation. Specifically, based on their efficacy in removing Aβ plaques from the brains of patients with AD, the U.S. Food and Drug Administration has approved three anti-amyloid MABs, aducanumab (Aduhelm®), lecanemab (Leqembi®), and donanemab (Kisunla™). Notably, lecanemab received traditional approval after demonstrating clinical benefit, supporting the Aβ cascade hypothesis. These MABs targeting Aβ are categorized based on their affinity to diverse conformational features of Aβ, including monomer, fibril, protofibril, and plaque forms of Aβ as well as pyroglutamate Aβ. First-generation MABs targeting the non-toxic monomeric Aβ, such as solanezumab, bapineuzumab, and crenezumab, failed to demonstrate clinical benefit for AD in clinical trials. In contrast, second-generation MABs, including aducanumab, lecanemab, donanemab, and gantenerumab directed against pathogenic Aβ species and aggregates have shown that reducing Aβ deposition can be an effective strategy to slow cognitive impairment in AD. In this review, we provide a comprehensive overview of the current status, mechanisms, outcomes, and limitations of second-generation MABs for the clinical treatment of AD. Moreover, we discuss the perspectives and future directions of anti-amyloid MABs in the treatment of AD.
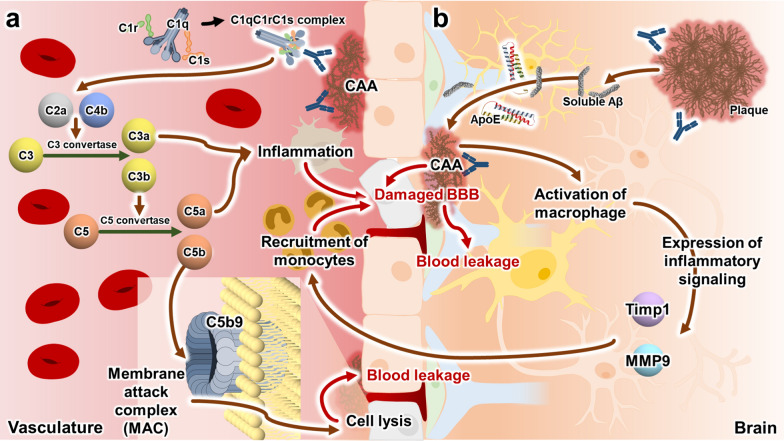
Keywords: Aducanumab; Alzheimer’s disease; Amyloid-related imaging abnormalities; Donanemab; Gantenerumab; Lecanemab.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not Applicable. Competing interests: Authors declare no competing interests.
Figures
References
-
- Kohler G, Milstein C. Continuous cultures of fused cells secreting antibody of predefined specificity. Nature. 1975;256(5517):495–7. - PubMed
-
- Breedveld FC. Therapeutic monoclonal antibodies. Lancet. 2000;355(9205):735–40. - PubMed
-
- Todd PA, Brogden RN. Muromonab CD3 A review of its pharmacology and therapeutic potential. Drugs. 1989;37(6):871–99. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
