

Interventricular septal dissection secondary to acute inferior myocardial infarction: case series and literature review
- PMID: 39865291
- PMCID: PMC11771034
- DOI: 10.1186/s13019-024-03271-z
Interventricular septal dissection secondary to acute inferior myocardial infarction: case series and literature review
Abstract
Background: Interventricular septal dissection is a critical disease characterized by the separation of the intraventricular septum into two layers, forming an intermediate layer with a cystic cavity that communicates with the root of the aorta or ventricle. It has low morbidity and high mortality rates.
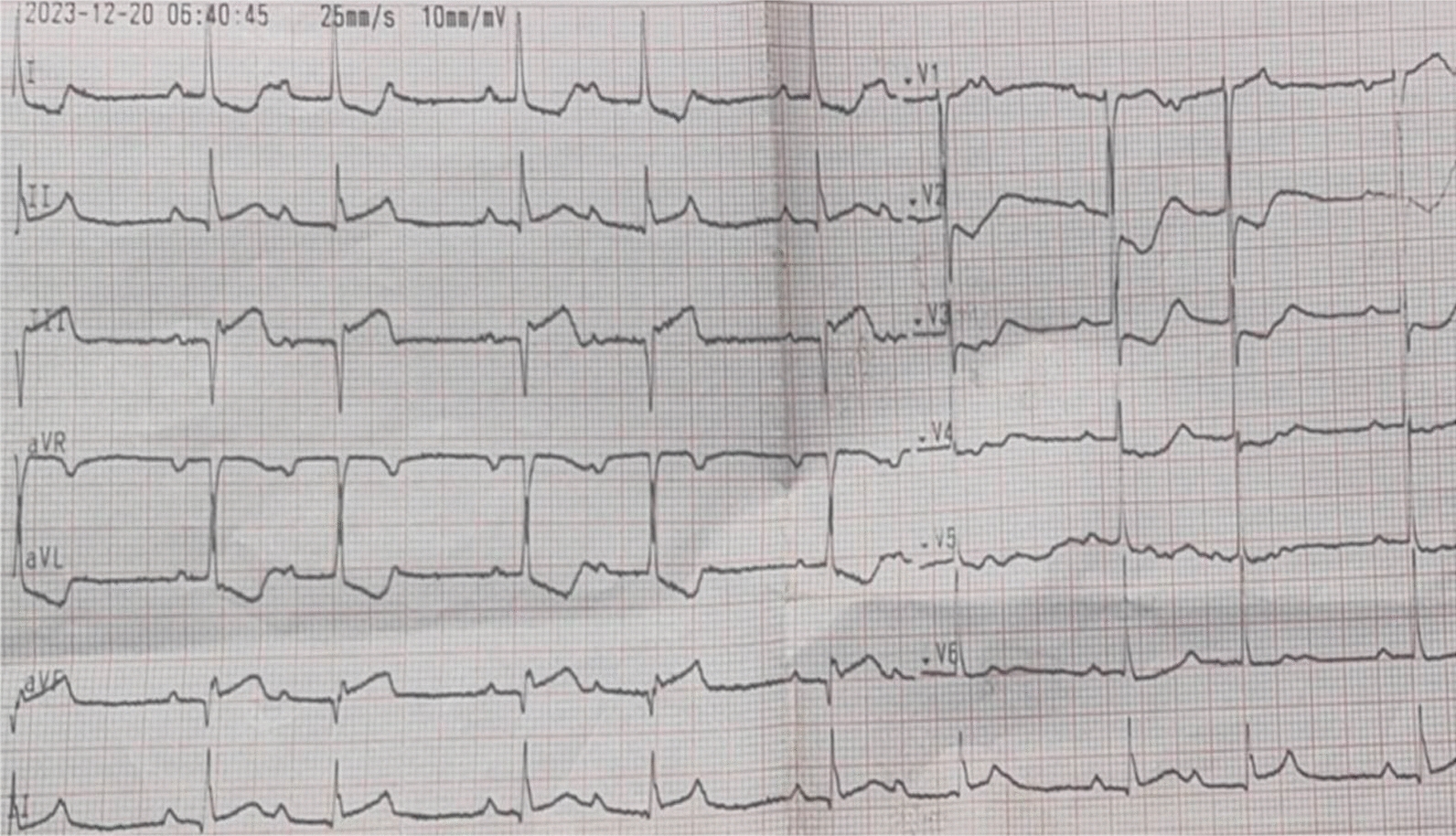
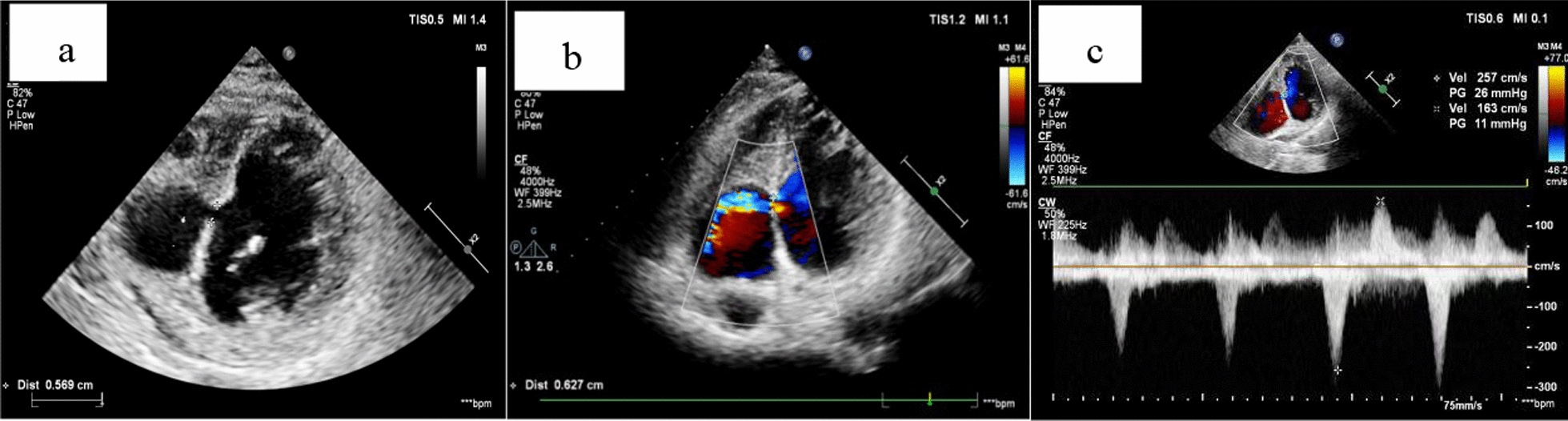
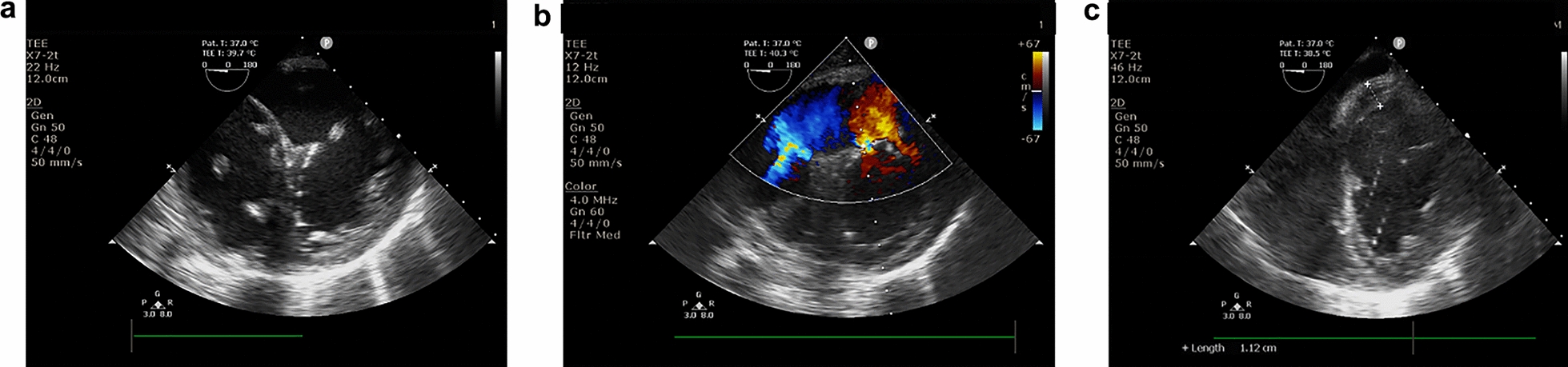
Case presentation: Case 1: A 58-year-old male with a history of hypertension and smoking presented to a local hospital due to chest tightness and pain for 4 days. Coronary angiography revealed diffuse lesions from the proximal to the middle segment of the left circumflex branch, with 80% stenosis at its most severe point, and complete occlusion of the proximal segment of the right coronary artery. A stent was implanted in the middle of the right coronary artery. Three months later, the patient was misdiagnosed with an aneurysm of the membranous ventricular septum with defect via echocardiography at the local hospital. After the implantation of a stent in the left circumflex branch, the patient came to our hospital for further diagnosis and treatment. The first ultrasound of our hospital misdiagnosed it as ventricular septal rupture, and a senior ultrasound doctor diagnosed the patient with interventricular septal dissection secondary to myocardial infarction. The patient underwent follow-up echocardiography every 1-2 months for 6 months. The patient remains asymptomatic with stable hemodynamics. The original treatment regimen and follow-up continues. Case 2: A 70-year-old male was admitted to a local hospital due to repeated chest distress for more than 20 years that worsened over several hours. Coronary angiography revealed complete occlusion of the right coronary artery. Cardiogenic shock occurred after percutaneous coronary intervention. The initial several echocardiography of the local hospital and our hospital misdiagnosed it as interventricular septal rupture secondary to myocardial infarction. The later echocardiography diagnosed it as interventricular septal dissection with rupture secondary to myocardial infarction. The patient underwent interventricular septal repair and mitral valvuloplasty after 25 days of medical treatment and died of multiple organ failure on the fourth day after the operation.
Conclusions: These two cases illustrate a complication of acute myocardial infarction and highlight the importance of echocardiography in its diagnosis. By exploring the etiology, pathogenesis, and key diagnostic points of IVSD, this study aims to provide valuable insights for clinical practice.
Keywords: Echocardiography; Interventricular septal dissection; Interventricular septal rupture; Myocardial infarction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Patient consent statement: The patient in case 1 and the legal client of patient in case 2 authorized the study, both of whom signed the written authorization consent form. Ethical approval and consent to participate: Patients signed an informed consent process that was reviewed by the Ethics Committee of Zhejiang University, which certified that the study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki. Competing interest: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Figures

Similar articles
-
Delayed ventricular septal rupture complicating acute inferior wall myocardial infarction.BMC Res Notes. 2013 Mar 28;6:124. doi: 10.1186/1756-0500-6-124. BMC Res Notes. 2013. PMID: 23537320 Free PMC article.
-
Transcatheter closure of ventricular septal rupture with prolonged support of intra-aortic balloon pump after primary PCI: a case report.BMC Cardiovasc Disord. 2021 Dec 18;21(1):605. doi: 10.1186/s12872-021-02392-w. BMC Cardiovasc Disord. 2021. PMID: 34922437 Free PMC article.
-
Ventricular septal rupture and right ventricular intramyocardial dissection secondary to acute inferior myocardial infarction.J Cardiovasc Comput Tomogr. 2010 Sep-Oct;4(5):342-4. doi: 10.1016/j.jcct.2010.05.019. Epub 2010 Jun 8. J Cardiovasc Comput Tomogr. 2010. PMID: 20638355
-
Ventricular septal rupture with right ventricular wall dissection after inferior ventricular infarction: A case report and literature review.J Clin Ultrasound. 2019 May;47(4):247-252. doi: 10.1002/jcu.22684. Epub 2019 Jan 4. J Clin Ultrasound. 2019. PMID: 30614010 Review.
-
[Myocardial dissection in infarction of the right ventricle. Clinical echocardiographic and pathological aspects].Arch Mal Coeur Vaiss. 1992 Apr;85(4):423-8. Arch Mal Coeur Vaiss. 1992. PMID: 1642502 Review. French.
References
-
- Fennich H, Doghmi N, Rim F, Belhaj S, Cheikhi F, Cherti M. Spontaneous rupture of right aortic sinus of Valsalva leading to massive cystic dissection of interventricular septum and complete heart block. Echocardiography. 2018;35(12):2109–12. 10.1111/echo.14166. - PubMed
-
- Stróżyk A, Kołaczkowska M, Fijałkowska J, Siondalski P, Fijałkowski M. Sinus of Valsalva rupture in a patient with a mechanical aortic prosthesis: aneurysm dissecting into the interventricular septum. Kardiol Pol. 2018;76(12):1742. 10.5603/KP.2018.0235. - PubMed
-
- Li HY, Wang M, Zhang WF, Wu JT, Wang TY, Sheng W, Niu ZZ. Diagnosis, treatment and follow-up analysis of 6 cases of dissecting aneurysm of the interventricular septum. Chin J Cardiovasc. 2021;26(5):463–7. 10.3969/j.issn.1007-5410.2021.05.012.
-
- Wu Q, Jin YP, Zhou L, Liu YF, Wu DZ. A dissecting aneurysm of interventricular septum resulting from congenital coronary artery fistula. J Clin Ultrasound. 2019;47(1):55–8. 10.1002/jcu.22639. - PubMed
-
- Huang ZX, Pu ZX, Shentu W, Li J, Shen ZH, Tan YB, Cheng L. A case report of asymptomatic right coronary fistula with giant interventricular aneurysm. Chin J Cardiol. 2019;47(6):496–7. 10.3760/cma.j.issn.0253-3758.2019.06.014. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
