

Diagnosis and management of de novo non-specific spinal infections: European Association of Neurosurgical Societies (EANS) Spine Section Delphi consensus recommendations
- PMID: 39866360
- PMCID: PMC11763570
- DOI: 10.1016/j.bas.2024.104178
Diagnosis and management of de novo non-specific spinal infections: European Association of Neurosurgical Societies (EANS) Spine Section Delphi consensus recommendations
Abstract
Introduction: The management of de novo non-specific spinal infections (spondylodiscitis - SD) remains inconsistent due to varying clinical practices and a lack of high-level evidence, particularly regarding the indications for surgery.
Research question: This study aims to develop consensus recommendations for the diagnosis and management of SD, addressing diagnostic modalities, surgical indications, and treatment strategies.
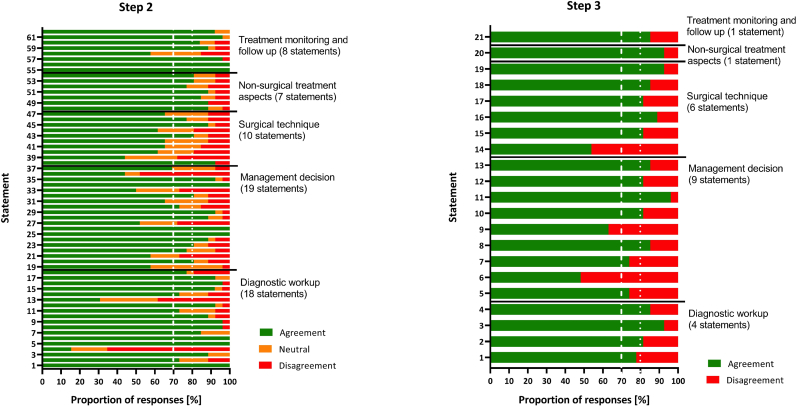
Material and methods: A Delphi process was conducted with 26 experts from the European Association of Neurosurgical Societies (EANS). Sixtytwo statements were developed on diagnostic workup, management decisions, surgical techniques, non-surgical treatment, and follow-up and submitted to the panel of experts.
Results: Consensus was reached on 38 of 62 statements. MRI was confirmed as the gold standard for diagnosis. Regarding surgical indications, the panel agreed that any new neurological deficit, even subtle, warrants surgical consideration. Motor deficits with a motor score (MRC) below 4 and bladder or bowel dysfunction were unanimously considered clear indications for surgery. For spinal deformity and instability, thresholds such as kyphosis >20°, scoliosis >10°, and vertebral body collapse >50% were established to guide surgical decision-making. Minimally invasive surgery (MIS) was endorsed whenever feasible, and a 12 week antibiotic treatment regimen was favored in cases of complicated infections.
Discussion and conclusion: This EANS consensus provides updated recommendations for SD management, incorporating recent evidence on improved outcomes with surgical therapy. While these guidelines offer a more structured approach to clinical decision-making, further research is required to optimize surgical timing and validate the long-term impact of these treatment strategies.
Keywords: Consensus; De novo spinal infection; Discitis; Non-specific; Pyogenic; Spinal osteomyelitis; Spondylodiscitis.
© 2024 Published by Elsevier B.V. on behalf of EUROSPINE, the Spine Society of Europe, EANS, the European Association of Neurosurgical Societies.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


Similar articles
-
Ongoing decision-making dilemma for treatment of de novo spinal infections: a comparison of the Spinal Infection Treatment Evaluation Score with the Spinal Instability Spondylodiscitis Score and Spine Instability Neoplastic Score.J Neurosurg Spine. 2024 May 17;41(2):273-282. doi: 10.3171/2024.2.SPINE23664. Print 2024 Aug 1. J Neurosurg Spine. 2024. PMID: 38759240
-
Variation of practice in the treatment of pyogenic spondylodiscitis: a European Association of Neurosurgical Societies Spine Section study.J Neurosurg Spine. 2024 May 17;41(2):263-272. doi: 10.3171/2024.2.SPINE231202. Print 2024 Aug 1. J Neurosurg Spine. 2024. PMID: 38759237
-
Early management of adult traumatic spinal cord injury in patients with polytrauma: a consensus and clinical recommendations jointly developed by the World Society of Emergency Surgery (WSES) & the European Association of Neurosurgical Societies (EANS).World J Emerg Surg. 2024 Jan 18;19(1):4. doi: 10.1186/s13017-023-00525-4. World J Emerg Surg. 2024. PMID: 38238783 Free PMC article.
-
Developing consensus for the management of pediatric cervical spine disorders and stabilization: a modified Delphi study.J Neurosurg Pediatr. 2022 Oct 28;31(1):32-42. doi: 10.3171/2022.9.PEDS22319. Print 2023 Jan 1. J Neurosurg Pediatr. 2022. PMID: 36308472 Review.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
References
-
- Appalanaidu N., Shafafy R., Gee C., et al. Predicting the need for surgical intervention in patients with spondylodiscitis: the Brighton Spondylodiscitis Score (BSDS) Eur. Spine J. 2019;28(4):751–761. - PubMed
-
- Arbelaez A., Restrepo F., Castillo M. Spinal infections: clinical and imaging features. Top. Magn. Reson. Imag. 2014;23(5):303–314. - PubMed
-
- Berbari E.F., Kanj S.S., Kowalski T.J., et al. Infectious diseases society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin. Infect. Dis. 2015;61(6):e26–e46. 2015. - PubMed
-
- Bernard L., Dinh A., Ghout I., et al. Antibiotic treatment for 6 weeks versus 12 weeks in patients with pyogenic vertebral osteomyelitis: an open-label, non-inferiority, randomised, controlled trial. Lancet. 2015;385(9971):875–882. - PubMed
-
- Dunbar J.A., Sandoe J.A., Rao A.S., Crimmins D.W., Baig W., Rankine J.J. The MRI appearances of early vertebral osteomyelitis and discitis. Clin. Radiol. 2010;65(12):974–981. - PubMed
LinkOut - more resources
Full Text Sources
