

Comparison of 12- to 24-Hour Versus 72-Hour Intravenous Terlipressin in Patients With Acute Esophageal Variceal Bleeding: A Systematic Review and Meta-analysis
- PMID: 39866669
- PMCID: PMC11758437
- DOI: 10.1177/87551225241311444
Comparison of 12- to 24-Hour Versus 72-Hour Intravenous Terlipressin in Patients With Acute Esophageal Variceal Bleeding: A Systematic Review and Meta-analysis
Abstract
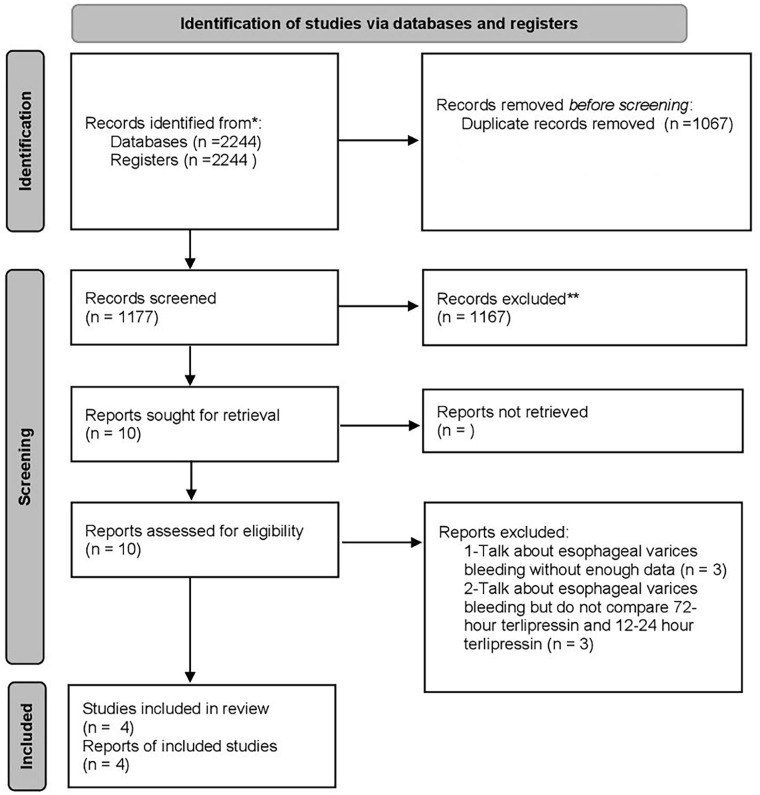
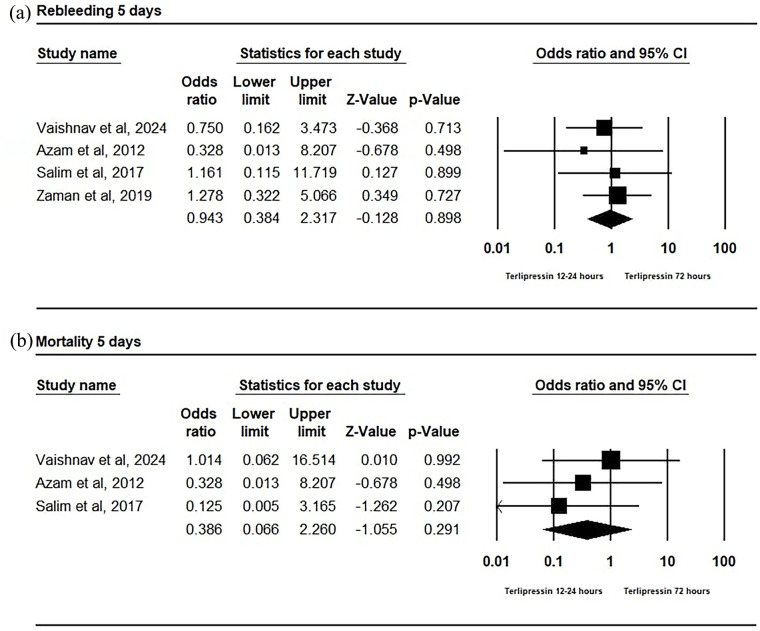
Objective: To compare the efficacy and safety of 12-24 hours versus 72 hours of intravenous terlipressin therapy in patients with acute esophageal variceal bleeding (AVB). Data sources: A systematic search was conducted using PubMed, Scopus, Cochrane Library, Google Scholar, Web of Science, VHL, and ClinicalTrials.gov for studies published up to February 24, 2024. The search terms included "terlipressin," "variceal bleeding," "short-course," and "72-hour treatment." Study selection and data extraction: Randomized controlled trials (RCTs) comparing 12 to 24 hours with 72 hours of terlipressin therapy in patients with AVB were included. Studies not meeting these criteria or focusing on unrelated outcomes were excluded. Two authors conducted data extraction and bias assessment independently, with discrepancies resolved by a third reviewer. Baseline characteristics and outcomes (rebleeding and mortality within 5 days) were recorded. Results: Four RCTs with 469 patients were included in the analysis. There were no significant differences observed in 5-day rebleeding rates (OR = 0.943; 95% CI [0.384, 2.317]; P = 0.898) or mortality rates (OR = 0.386; 95% CI [0.066, 2.260]; P = 0.291) between terlipressin treatment durations of 12 to 24 hours and 72 hours within the first 5 days posttreatment. In addition, no heterogeneity was found in both variables (P > 0.1). Conclusion: This meta-analysis indicates that there is no significant difference in rebleeding rates or mortality between 12 to 24 hours and 72 hours of terlipressin therapy for AVB within 5 days posttreatment. Shorter treatment durations may offer advantages in terms of resource utilization and adverse event risk but require further validation through studies involving larger patient populations.
Keywords: bleeding; esophageal variceal; meta-analysis; terlipressin; vasopressors.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Comparison of 1-day versus 3-day intravenous terlipressin in cirrhosis patients with variceal bleeding: A pilot randomised controlled trial.Aliment Pharmacol Ther. 2024 Mar;59(5):645-655. doi: 10.1111/apt.17868. Epub 2024 Jan 7. Aliment Pharmacol Ther. 2024. PMID: 38186012 Clinical Trial.
-
[Comparison of terlipressin and octreotide with variceal ligation for controlling acute esophageal variceal bleeding--a randomized prospective study].Korean J Hepatol. 2006 Sep;12(3):385-93. Korean J Hepatol. 2006. PMID: 16998290 Clinical Trial. Korean.
-
Terlipressin for the treatment of acute variceal bleeding: A systematic review and meta-analysis of randomized controlled trials.Medicine (Baltimore). 2018 Nov;97(48):e13437. doi: 10.1097/MD.0000000000013437. Medicine (Baltimore). 2018. PMID: 30508958 Free PMC article.
-
The effect of shortening vasoactive drug durations alongside endoscopic therapy in esophageal variceal bleeding: an updated systematic review and meta-analysis.Ann Gastroenterol. 2024 Sep-Oct;37(5):567-578. doi: 10.20524/aog.2024.0906. Epub 2024 Aug 19. Ann Gastroenterol. 2024. PMID: 39238793 Free PMC article.
-
Vasoactive Agents for the Management of Acute Variceal Bleeding: A Systematic Review and Meta-analysis.J Gastrointestin Liver Dis. 2021 Mar 13;30(1):110-121. doi: 10.15403/jgld-3191. J Gastrointestin Liver Dis. 2021. PMID: 33723542
References
-
- Grace ND. Diagnosis and treatment of gastrointestinal bleeding secondary to portal hypertension. American College of Gastroenterology Practice Parameters Committee. Am J Gastroenterol. 1997;92(7):1081-1091. - PubMed
Publication types
LinkOut - more resources
Full Text Sources