

THE ROLE OF PLASMA COPEPTIN LEVEL IN DETERMINING THE SEVERITY AND MORTALITY OF SUBARACHNOID HEMORRHAGE
- PMID: 39866759
- PMCID: PMC11759122
- DOI: 10.20471/acc.2023.62.04.3
THE ROLE OF PLASMA COPEPTIN LEVEL IN DETERMINING THE SEVERITY AND MORTALITY OF SUBARACHNOID HEMORRHAGE
Abstract
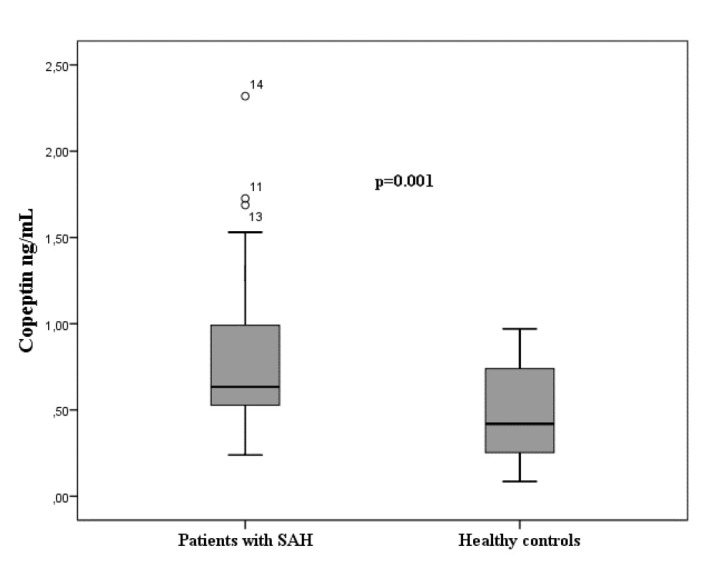
The study aimed to investigate the role of plasma copeptin level in setting the diagnosis, severity and mortality of patients with subarachnoid hemorrhage (SAH) admitted to the emergency department. We included patients aged ≥18 years who were diagnosed with SAH. Blood samples were collected from patients at the time of admission to the emergency department for assessment of plasma copeptin levels. The Glasgow Coma Scale (GCS), World Federation of Neurological Surgeons (WFNS), modified Fisher score, in-hospital mortality and one-year mortality rates were determined in patients. There was a statistically significant difference in plasma copeptin levels between the patients (mean: 0.78±0.41 ng/mL) and healthy controls (mean: 0.48±0.27 ng/mL) (p=0.001). There was no significant correlation of plasma copeptin levels with the GCS, WFNS, and modified Fisher scores. There was no significant difference in copeptin levels between the patients who died in the hospital (mean: 0.73±0.42 ng/mL) and those who did not (mean: 0.80±0.41 ng/mL) (p=0.41). Although plasma copeptin level may be used in the diagnosis of SAH, it does not have a role in determining the patient condition severity and mortality.
Keywords: Copeptin; Emergency department; Mortality; Subarachnoid haemorrhage.
Sestre Milosrdnice University Hospital.
Figures


References
-
- Galea J, Ogungbenro K, Hulme S, Patel H, Scarth S, Hoadley M, et al. Reduction of inflammation after administration of interleukin-1 receptor antagonist following aneurysmal subarachnoid hemorrhage: results of the subcutaneous interleukin-1Ra in SAH (SCIL-SAH) study. J Neurosurg. 2018;128:515–23. Epub 2017 Feb 24.10.3171/2016.9.JNS16615 - DOI - PubMed
-
- Hackman JL, Nelson AM, Ma OJ. Spontaneous subarachnoid and intracerebral hemorrhage. In: Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM (eds). Emergency Medicine A Comprehensive Study Guide. 8th edn. New York: The Mc Graw Hill Companies, 2016; pp. 1137-41.
-
- Novaković N, Lepić M, Minić L, Radenović K, Rotim A, Rasulić L. Combined treatment of ruptured middle cerebral artery aneurysm followed by subarachnoid hemorrhage and acute subdural hematoma in multiple aneurysm disease of cerebral blood vessels: case report. Acta Clin Croat. 2016;55:659–62. 10.20471/acc.2016.55.04.19 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources