

U-shaped association between the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and mortality risk in obese adults: evidence from NHANES 1999-2018
- PMID: 39866802
- PMCID: PMC11759299
- DOI: 10.3389/fcvm.2024.1524465
U-shaped association between the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and mortality risk in obese adults: evidence from NHANES 1999-2018
Abstract
Background: Obesity, often accompanied by dyslipidemia and increased cardiovascular risk, poses a significant threat to overall mortality. The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) has been identified as a valuable parameter for assessing dyslipidemia. The goal of the study was to elucidate the relationship between NHHR and mortality in obese populations.
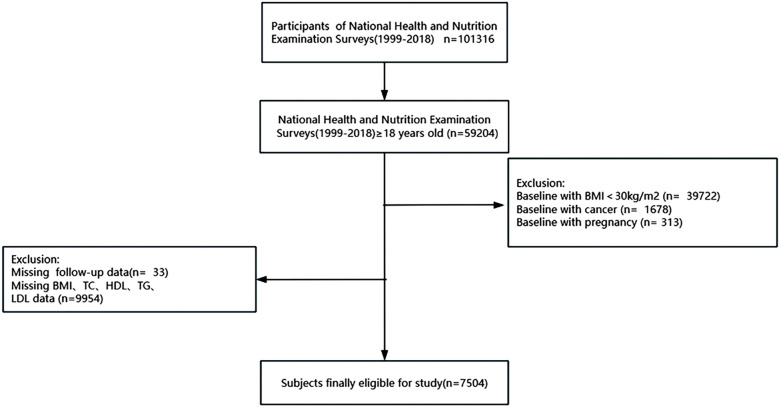
Methods: Data for the study cohort were sourced from the National Health and Nutrition Examination Survey (1999-2018). The association between NHHR and mortality from all causes and cardiovascular disease was examined through multivariable Cox regression and restricted cubic splines (RCS). Segmented multivariable Cox regression and subgroup analyses were conducted when segmented effects were identified. The reliability of the results was confirmed through multiple sensitivity analyses.
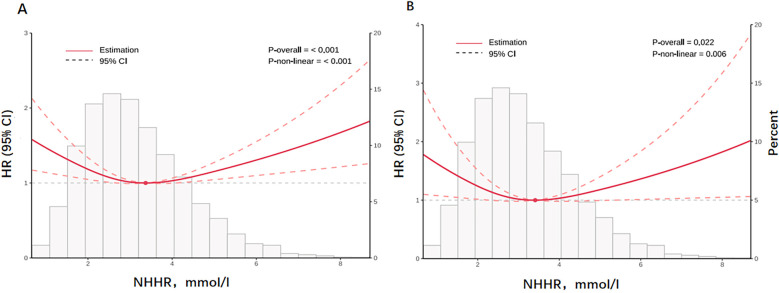
Results: A total of 7,504 participants were included in the analysis. During a median follow-up of 119 months, 866 subjects died for all causes, of which 318 were related to cardiovascular diseases. A U-shaped association was found utilizing RCS analysis, with cardiovascular mortality and all-cause mortality exhibiting the lowest risk points at 3.409 and 3.369, respectively. The fully adjusted model revealed a negative relationship between the risk of cardiovascular mortality (HR = 0.68, 95% CI: 0.49-0.94) and all-cause mortality (HR = 0.82, 95% CI: 0.67-1.00) for per 1 mmol/L increase in NHHR levels below the cut-off value. On the other hand, above the cut-off point, NHHR was positively correlated with cardiovascular mortality (HR = 1.18, 95% CI: 1.02-1.36) and all-cause mortality (HR = 1.13, 95% CI: 1.01-1.28). The sensitivity results of this study were in accordance with earlier findings, and no significant interactions in NHHR levels were discovered across different subgroups.
Conclusions: In the obese adults, NHHR displayed a U-shaped relationship with cardiovascular and all-cause death. Monitoring and managing NHHR levels in obese population may help mitigate the risk of mortality.
Keywords: American adults; Non-HDL-C/HDL-C; all-cause mortality; cardiovascular mortality; obesity.
© 2025 Lin, Yi, Hu, Chen and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) as a predictor of all-cause and cardiovascular mortality in US adults with diabetes or prediabetes: NHANES 1999-2018.BMC Med. 2024 Aug 7;22(1):317. doi: 10.1186/s12916-024-03536-3. BMC Med. 2024. PMID: 39113030 Free PMC article.
-
Non-high density lipoprotein cholesterol/high density lipoprotein cholesterol is L-shaped associated with all-cause mortality and U-shaped with cardiovascular mortality in hypertensive patients.Front Endocrinol (Lausanne). 2025 Mar 13;16:1490229. doi: 10.3389/fendo.2025.1490229. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40182639 Free PMC article.
-
The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio as a predictor of all cause and cardiovascular mortality in United States adults with NAFLD: a prospective cohort study.BMC Gastroenterol. 2025 Apr 23;25(1):288. doi: 10.1186/s12876-025-03873-4. BMC Gastroenterol. 2025. PMID: 40269750 Free PMC article.
-
Predictive value of the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) for all-cause and cardiovascular mortality with non-hyperhomocysteinemia: evidence from NHANES 1999 to 2006.Front Nutr. 2025 May 20;12:1586558. doi: 10.3389/fnut.2025.1586558. eCollection 2025. Front Nutr. 2025. PMID: 40463467 Free PMC article.
-
Association of the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) with COPD prevalence and all-cause mortality: a population-based study based on NHANES 2007-2016.Front Med (Lausanne). 2025 Apr 3;12:1533744. doi: 10.3389/fmed.2025.1533744. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40248071 Free PMC article.
Cited by
-
Trends in dyslipidemia prevalence among Uyghur adults of different genders in China: a retrospective cohort study.PeerJ. 2025 May 2;13:e19344. doi: 10.7717/peerj.19344. eCollection 2025. PeerJ. 2025. PMID: 40330697 Free PMC article.
-
Non-linear correlation between the ratio of high-density lipoprotein cholesterol to C-reactive protein and all-cause mortality in adults: an extensive study based on nationwide data.Popul Health Metr. 2025 Jul 1;23(1):32. doi: 10.1186/s12963-025-00396-8. Popul Health Metr. 2025. PMID: 40597306 Free PMC article.
References
-
- Wormser D, Kaptoge S, Di Angelantonio E, Wood AM, Pennells L, Thompson A, et al. Separate and combined associations of body-mass index and abdominal adiposity with cardiovascular disease: collaborative analysis of 58 prospective studies. Lancet. (2011) 377(9771):1085–95. 10.1016/S0140-6736(11)60105-0 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources