

This is a preprint.
Hierarchical Neurocognitive Model of Externalizing and Internalizing Comorbidity
- PMID: 39866873
- PMCID: PMC11760247
- DOI: 10.21203/rs.3.rs-5397195/v1
Hierarchical Neurocognitive Model of Externalizing and Internalizing Comorbidity
Abstract
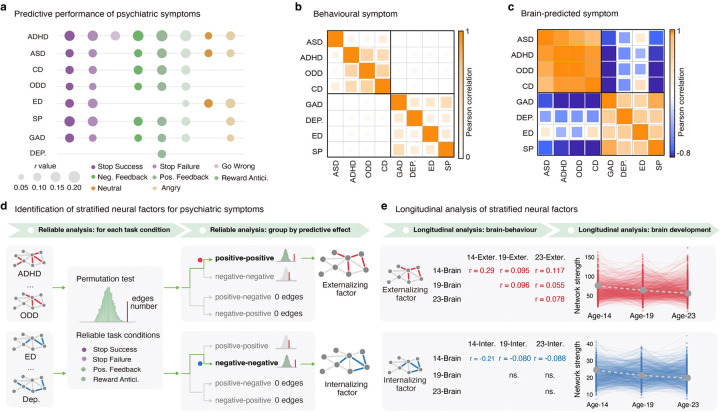
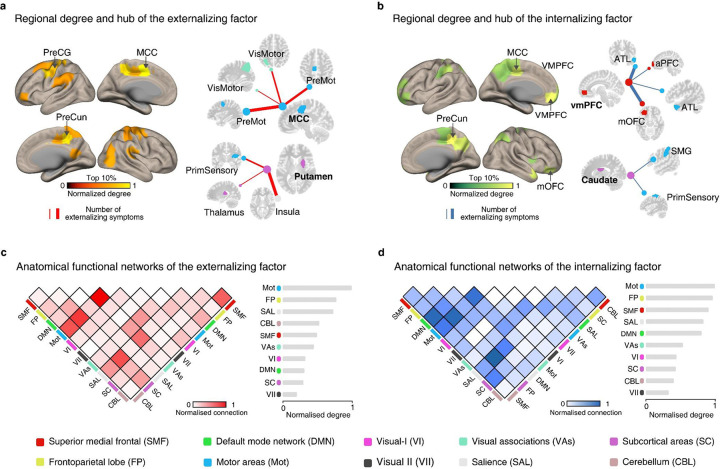
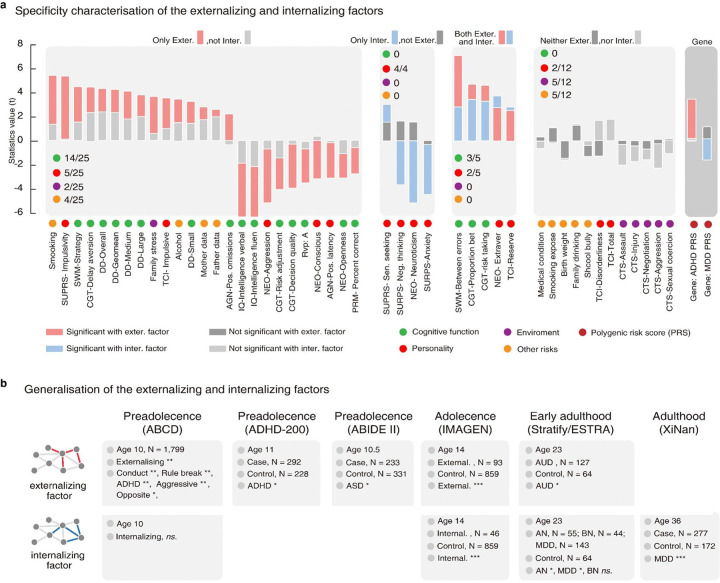
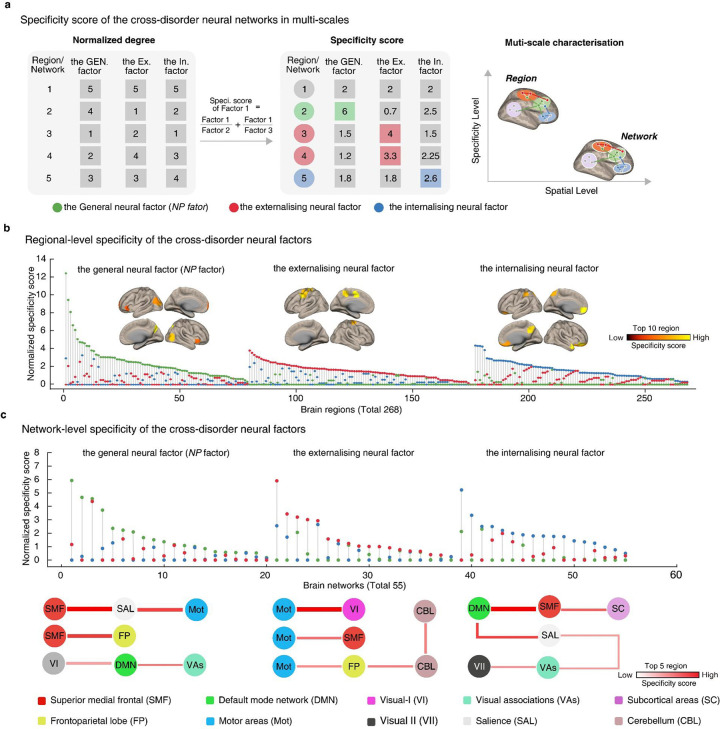
Mounting evidence suggests hierarchical psychopathology factors underlying psychiatric comorbidity. However, the exact neurobiological characterizations of these multilevel factors remain elusive. In this study, leveraging the brain-behavior predictive framework with a 10-year longitudinal imaging-genetic cohort (IMAGEN, ages 14, 19 and 23, N = 1,750), we constructed two neural factors underlying externalizing and internalizing symptoms, which were reproducible across six clinical and population-based datasets (ABCD, STRATIFY/ESTRA, ABIDE II, ADHD-200 and XiNan, from age 10 to age 36, N = 3,765). These two neural factors exhibit distinct neural configurations: hyperconnectivity in impulsivity-related circuits for the externalizing symptoms and hypoconnectivity in goal-directed circuits for the internalizing symptoms. Both factors also differ in their cognitive-behavior relevance, genetic substrates and developmental profiles. Together with previous studies, these findings propose a hierarchical neurocognitive spectral model of comorbid mental illnesses from preadolescence to adulthood: a general neuropsychopathological (NP) factor (manifested as inefficient executive control) and two stratified factors for externalizing (deficient inhibition control) and internalizing (impaired goal-directed function) symptoms, respectively. These holistic insights are crucial for the development of stratified therapeutic interventions for mental disorders.
Conflict of interest statement
Additional Declarations: Yes there is potential Competing Interest. T.B. served in an advisory or consultancy role for Lundbeck, Medice, Neurim Pharmaceuticals, Oberberg GmbH and Shire. He received conference support or speaker’s fee from Lilly, Medice, Novartis and Shire. He has been involved in clinical trials conducted by Shire and Viforpharma. He received royalties from Hogrefe, Kohlhammer, CIP Medien and Oxford University Press. The present work is unrelated to the above grants and relationships. G.J.B. received honoraria from General Electric Healthcare for teaching scanner programming courses. All other authors declare no competing interests. GJB received honoraria for teaching from GE Healthcare
Figures

References
-
- Rodriguez-Seijas C., et al. Diversity and the Hierarchical Taxonomy of Psychopathology (HiTOP). Nature Reviews Psychology (2023).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
