

Recurrent Poorly Differentiated Thyroid Cancer Successfully Treated With Radiation and Immunotherapy
- PMID: 39866918
- PMCID: PMC11758140
- DOI: 10.1210/jcemcr/luaf015
Recurrent Poorly Differentiated Thyroid Cancer Successfully Treated With Radiation and Immunotherapy
Abstract
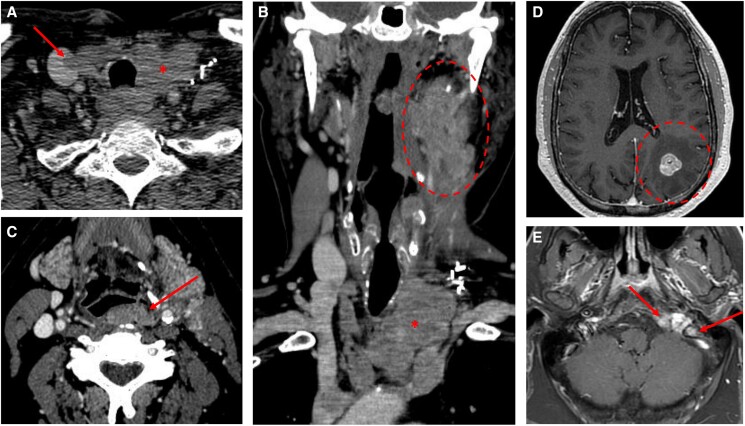
A 65-year-old patient presented with recurrent, locally advanced poorly differentiated thyroid cancer despite 2 neck surgeries, and with newly diagnosed brain and skull base metastases. He was treated with palliative stereotactic radiosurgery to the brain and skull base lesions. Thereafter, as no targetable genetic alteration was identified and antiangiogenic multikinase inhibitors were deemed at high risk of hemorrhagic complications, off-label systemic therapies were considered. The mechanistic target of rapamycin (mTOR) inhibitor everolimus could not be obtained due to lack of insurance coverage, so the patient was treated with single-agent pembrolizumab. He showed an initial remarkable response, but unfortunately had disease progression in the neck and upper mediastinum after 1 year of therapy. At that time, he was treated with external beam radiotherapy, with concomitant pembrolizumab. He was then found to have an CTSB::ALK fusion, which has previously been described in 2 cases of thyroid cancer. However, as he showed a positive response to radiation with pembrolizumab, he continued single-agent immune checkpoint inhibition and had a persistent marked response almost a year after completing radiation. The patient was then followed at an outside institution and was transitioned to hospice at time of progression per his preference. He died 4 years after his initial diagnosis.
Keywords: ALK fusion; immunotherapy; pembrolizumab; poorly differentiated thyroid cancer; radiation therapy; synergy.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures


References
-
- Christofer Juhlin C, Mete C, Baloch ZW. The 2022 WHO classification of thyroid tumors: novel concepts in nomenclature and grading. Endocr Relat Cancer. 2023;30(2):e220293. - PubMed
-
- Fagin JA, Wells SA Jr. Biologic and clinical perspectives on thyroid cancer. N Engl J Med. 2016;375(11):2306‐2307. - PubMed
-
- Hamidi S, Dadu R, Busaidy NL, et al. Cobimetinib plus atezolizumab for RAS and NF1/2-mutated poorly differentiated thyroid carcinoma. J Clin Oncol. 2024;42(16_suppl):6106‐6106.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous