

A Novel Approach to Potentially Improving Soft-Tissue Sarcoma Survival: Prophylactic Lung Radiotherapy Inhibits Growth of Lung Metastases and Prolongs Survival in a Murine Soft-Tissue Sarcoma Model
- PMID: 39867071
- PMCID: PMC11757009
- DOI: 10.7759/cureus.76334
A Novel Approach to Potentially Improving Soft-Tissue Sarcoma Survival: Prophylactic Lung Radiotherapy Inhibits Growth of Lung Metastases and Prolongs Survival in a Murine Soft-Tissue Sarcoma Model
Abstract
Background: Circulating tumor cells and clusters (CTC) from soft-tissue sarcoma (STS) that become entrapped in the lung can form micro-metastases and lead to pulmonary metastatic disease. Many patients with localized high-risk STS later develop metastases. Radiation is effective at reducing local recurrence by eradicating microscopic infiltration and satellites in the reactive zone surrounding the primary tumor. Prophylactic lung irradiation for patients with high-risk STS is a novel concept to potentially reduce the appearance of macroscopic metastases and improve survival. A proof-of-principle study was performed based on a novel approach: prophylactic lung radiation after resection of the primary tumor to address microscopic pulmonary deposits from CTC.
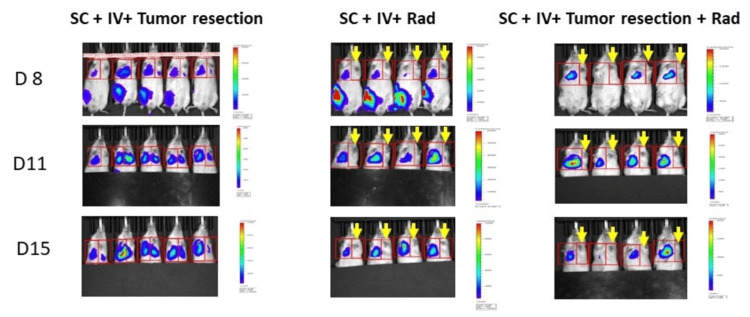
Methods: Immunocompromised mice and luciferase-expressing human fibrosarcoma (HT-1080-Luc) cell lines were used. In phase 1, HT-1080-Luc cells were injected into the tail vein to simulate CTC for the development of pulmonary metastases. Whole-lung irradiation (WLI) was then performed in the treated mice prior to the appearance of macroscopic metastases. In phase 2, a flank tumor was established to simulate a primary STS, followed by a tail-vein injection of HT-1080-Luc cells. Treatment groups included surgical removal of the primary STS and hemithoracic irradiation (HTI). Body weight and bioluminescence data were obtained and the mice were euthanized on Day 31 (phase 1) and Day 15 (phase 2) or when they reached 20% weight loss.
Results: In phase 1, prophylactic WLI increased survival and decreased pulmonary metastases. In phase 2, prophylactic HTI (left lung) decreased pulmonary metastases compared to controls. Lung histology showed dramatically decreased growth and number of established metastases with HTI. Resection of the primary tumor did not affect the growth of metastases.
Conclusion: Prophylactic WLI after resection of the primary tumor to inhibit the growth of pulmonary metastases from previously entrapped CTCs may be a promising approach to improve survival for patients with localized high-risk STS.
Keywords: lung metastasis; murine model; prophylactic; radiation; soft-tissue sarcoma.
Copyright © 2024, Ruditsky et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: University of Maryland, Baltimore, Institutional Animal Care and Use Committee (IACUC) Issued protocol number 1021001. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures








References
-
- Incidence and survival in sarcoma in the United States: A focus on musculoskeletal lesions. Ng VY, Scharschmidt TJ, Mayerson JL, Fisher JL. https://pubmed.ncbi.nlm.nih.gov/23749914/ Anticancer Res. 2013;33:2597–2604. - PubMed
-
- Soft-tissue sarcoma in adults: An update on the current state of histiotype-specific management in an era of personalized medicine. Gamboa AC, Gronchi A, Cardona K. CA Cancer J Clin. 2020;70:200–229. - PubMed
-
- Soft tissue sarcoma presenting with metastatic disease: Outcome with primary surgical resection. Ferguson PC, Deheshi BM, Chung P, et al. Cancer. 2011;117:372–379. - PubMed
-
- Histologic assessment of peritumoral edema in soft tissue sarcoma. White LM, Wunder JS, Bell RS, et al. Int J Radiat Oncol Biol Phys. 2005;61:1439–1445. - PubMed
-
- Neo-adjuvant chemotherapy for primary high-grade extremity soft tissue sarcoma. Grobmyer SR, Maki RG, Demetri GD, Mazumdar M, Riedel E, Brennan MF, Singer S. Ann Oncol. 2004;15:1667–1672. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources