

Association of Immune Nutrition Indices with the Risk of All-Cause Mortality and Cardiovascular Mortality in Patients with Heart Failure in the NHANES (1999-2018)
- PMID: 39867204
- PMCID: PMC11759971
- DOI: 10.31083/RCM25055
Association of Immune Nutrition Indices with the Risk of All-Cause Mortality and Cardiovascular Mortality in Patients with Heart Failure in the NHANES (1999-2018)
Abstract
Background: Heart failure (HF) remains a global challenge with disappointing long-term outcomes. Malnutrition is prevalent in patients with HF and disrupts the equilibrium of immune and inflammatory responses, resulting in further deterioration of the HF. Novel indicators emerge as immune nutrition indices, including the prognostic nutritional index (PNI), neutrophil-to-lymphocyte ratio (NLR), Controlling Nutritional Status (CONUT) score, and cholesterol-modified prognostic nutritional index (CPNI). This study examines the correlation between immune nutrition indices and all-cause and cardiovascular mortality in patients with HF.
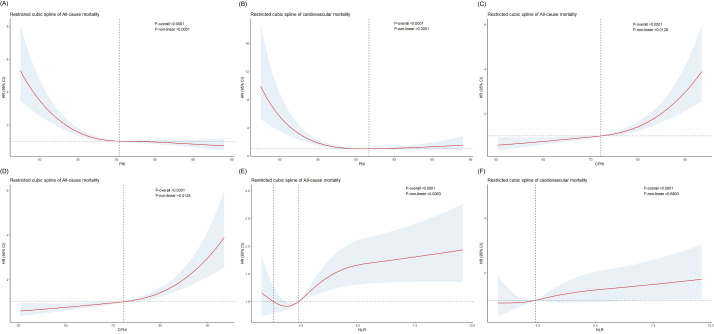
Methods: The data source for this study was the National Health and Nutrition Examination Survey (NHANES). A total of 1232 participants with HF were included. Weighted Cox proportional hazards models were employed to assess the independent association of different immune nutrition indices with mortality risk, alongside subgroup analyses and Kaplan-Meier survival curves. Restricted cubic spline analysis was utilized to clarify the detailed association between immune nutrition indices and hazard ratio (HR). A time-dependent receiver operating characteristic curve analysis was conducted to assess the predictive ability.
Results: After full adjustments, PNI is independently related to all-cause mortality (HR = 0.94, 95% CI: 0.92-0.97) and cardiovascular mortality (HR = 0.94, 95% CI: 0.90-0.99). CPNI, CONUT, and NLR also showed an independent association with the prognosis of HF. Time-dependent receiver operating characteristic curve analysis indicated that PNI exhibited the highest predictive power for mortality among the CPNI, CONUT, and NLR indexes.
Conclusions: Our study revealed that immune nutrition indicators, including CPNI, could predict all-cause mortality and cardiovascular mortality in the HF population. Compared with other indicators, PNI is the most effective predictor.
Keywords: all-cause mortality; cardiovascular mortality; heart failure; immune; inflammatory; nutrition.
Copyright: © 2025 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Davran GB, Davran AÇ, Karabag T. The relationship of prognostic nutritional index with prognosis and inflammation in patient with heart failure and reduced ejection fraction. Nutrition and Health . 2023;29:737–743. - PubMed
-
- Xu JP, Zeng RX, Zhang YZ, Lin SS, Tan JW, Zhu HY, et al. Systemic inflammation markers and the prevalence of hypertension: A NHANES cross-sectional study. Hypertension Research . 2023;46:1009–1019. - PubMed
-
- Ren J, Wang XY, Sun Y. Neutrophil-Lymphocyte Ratio Can be Used as a Predictor of Prognosis in Patients With Heart Failure. Angiology . 2023;33197231201927. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
