

Polymicrogyria in infants with symptomatic congenital cytomegalovirus at birth is associated with epilepsy: A retrospective, descriptive cohort study
- PMID: 39869483
- PMCID: PMC12237226
- DOI: 10.1111/dmcn.16250
Polymicrogyria in infants with symptomatic congenital cytomegalovirus at birth is associated with epilepsy: A retrospective, descriptive cohort study
Abstract
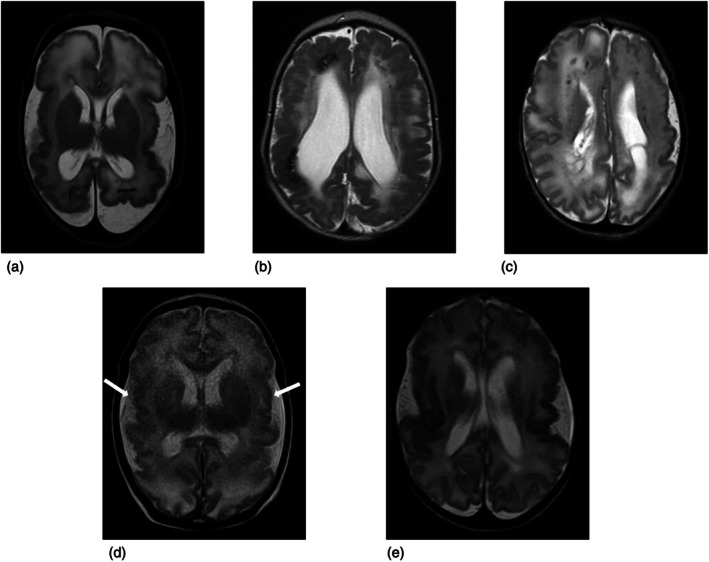
Aim: To identify neonatal magnetic resonance imaging (MRI) features that predict the likelihood of children with congenital cytomegalovirus (cCMV) developing epilepsy, together with clinical features and a validated MRI scoring system.
Method: This was a retrospective descriptive cohort study of infants with cCMV referred to a paediatric infectious disease centre between April 2012 and March 2022, and followed up for at least 2 years. MRI was performed before 4 months of age and assessed by two paediatric neuroradiologists.
Results: Ninety children with cCMV were included, 46 were female and 44 were male. The median age at MRI was 20 days, (standard deviation = 34, range = 1-200). Seventy-two of 90 children were symptomatic at birth and 7 of 72 developed epilepsy (9.7% of symptomatic infants, 7.8% of total). None of 18 asymptomatic children developed epilepsy. Those with epilepsy were more likely to be symptomatic at birth (100% vs. 76%, p = 0.14) and to have cortical malformations (86% vs. 15%, p < 0.001). Infants with polymicrogyria (PMG) were more likely to develop epilepsy (odds ratio = 35 [3.9-317.1], p < 0.001). A 1-year remission was achieved in three of seven children; four required multiple antiseizure medications without remission.
Interpretation: The strongest correlate of epilepsy development was PMG. Infants with symptomatic cCMV at birth and PMG were more likely to develop epilepsy, and were likely to require one or more antiseizure medications. Parents of infants with cCMV and cortical malformations should be counselled regarding this risk. Including PMG severity in cCMV MRI scoring could improve epilepsy risk prediction.
© 2025 The Author(s). Developmental Medicine & Child Neurology published by John Wiley & Sons Ltd on behalf of Mac Keith Press.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to declare.
Figures
Similar articles
-
Prognosis of adults and children following a first unprovoked seizure.Cochrane Database Syst Rev. 2023 Jan 23;1(1):CD013847. doi: 10.1002/14651858.CD013847.pub2. Cochrane Database Syst Rev. 2023. PMID: 36688481 Free PMC article.
-
Neurobehavioral outcomes of neonatal asymptomatic congenital cytomegalovirus infection at 12-months.J Neurodev Disord. 2024 Apr 18;16(1):19. doi: 10.1186/s11689-024-09533-0. J Neurodev Disord. 2024. PMID: 38637762 Free PMC article.
-
The value of magnetic resonance imaging in congenital cytomegalovirus infection: a systematic review.Pediatr Radiol. 2024 Dec;54(13):2157-2174. doi: 10.1007/s00247-024-06051-y. Epub 2024 Oct 18. Pediatr Radiol. 2024. PMID: 39419855
-
Palivizumab for immunoprophylaxis of respiratory syncytial virus (RSV) bronchiolitis in high-risk infants and young children: a systematic review and additional economic modelling of subgroup analyses.Health Technol Assess. 2011 Jan;15(5):iii-iv, 1-124. doi: 10.3310/hta15050. Health Technol Assess. 2011. PMID: 21281564 Free PMC article.
-
Impact of congenital cytomegalovirus infection on vestibular dysfunction and hearing outcomes in a cohort of children.Sci Rep. 2025 May 6;15(1):15740. doi: 10.1038/s41598-025-98150-5. Sci Rep. 2025. PMID: 40325024 Free PMC article.
Cited by
-
Congenital CMV infection and central nervous system involvement: mechanisms, treatment, and long-term outcomes.Eur J Pediatr. 2025 May 31;184(6):381. doi: 10.1007/s00431-025-06215-4. Eur J Pediatr. 2025. PMID: 40448827 Review.
References
-
- Lim Y, Lyall H. Congenital cytomegalovirus – who, when, what‐with and why to treat? J Infect. 2017. Jun;74:S89–94. - PubMed
-
- Bartlett AW, McMullan B, Rawlinson WD, Palasanthiran P. Hearing and neurodevelopmental outcomes for children with asymptomatic congenital cytomegalovirus infection: A systematic review. Rev Med Virol. 2017. Sep 1;27(5). - PubMed
-
- Leruez‐Ville M, et al. Consensus recommendation for prenatal, neonatal and postnatal management of congenital cytomegalovirus infection from the European congenital infection initiative (ECCI). The Lancet Regional Health ‐ Europe, (2024), 100892, 40. 10.1016/j.lanepe.2024.100892 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
