

Determination of adequate bony resection margins in inflammatory jaw pathologies using SPECT-CT in primary mandibular reconstruction with virtually planned vascularized bone flaps
- PMID: 39870950
- PMCID: PMC11772511
- DOI: 10.1007/s00784-025-06170-2
Determination of adequate bony resection margins in inflammatory jaw pathologies using SPECT-CT in primary mandibular reconstruction with virtually planned vascularized bone flaps
Abstract
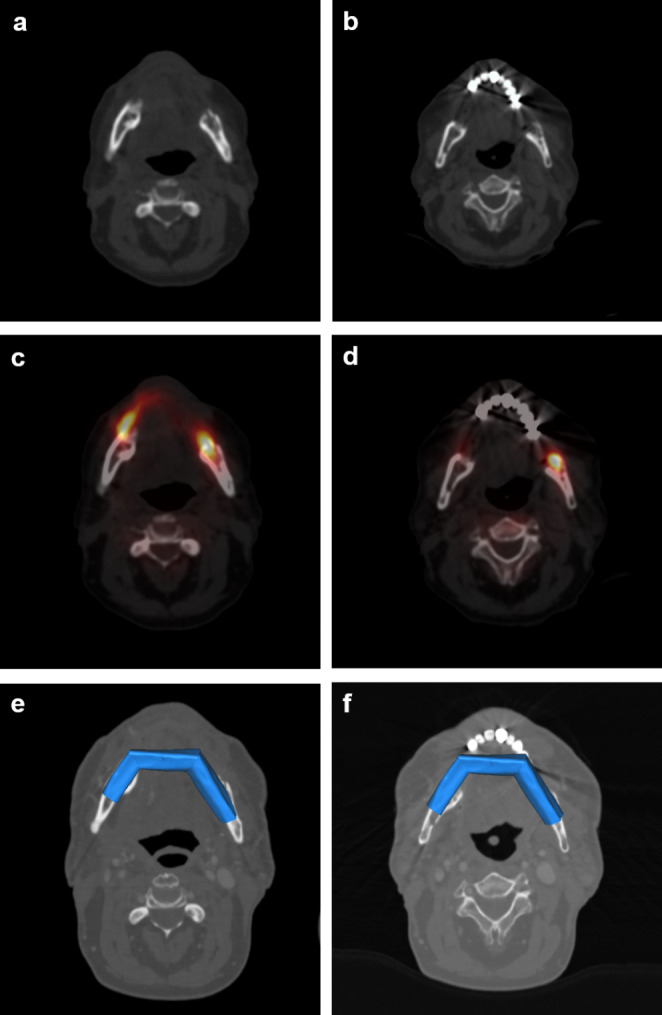
Objectives: In advanced stages of osteoradionecrosis, medication-related osteonecrosis of the jaw, and osteomyelitis, a resection of sections of the mandible may be unavoidable. The determination of adequate bony resection margins is a fundamental problem because bony resection margins cannot be secured intraoperatively. Single-photon emission computed tomography (SPECT-CT) is more accurate than conventional imaging techniques in detecting inflammatory jaw pathologies. The clinical benefit for virtual planning of mandibular resection and primary reconstruction with vascularized bone flaps has not yet been investigated. This study aimed to evaluate the determination of adequate bony resection margins using SPECT computed tomography (SPECT-CT) for primary microvascular reconstruction of the mandible in inflammatory jaw pathologies.
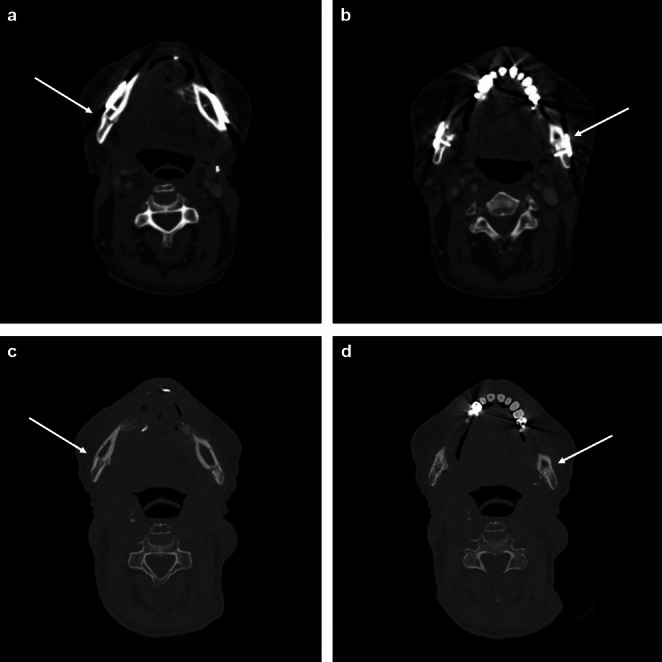
Materials and methods: The cases of 20 patients with inflammatory jaw pathologies who underwent primary microvascular mandibular reconstruction after the bony resection margins were determined with SPECT-CT were retrospectively analyzed. The bony resection margins determined by SPECT-CT were histologically validated. The sensitivity was calculated as the detection rate and the positive predictive value as the diagnostic precision. Radiological ossification of the vascularized bone flaps with the mandibular stumps was assessed at least 6 months after reconstruction. The clinical course was followed for 12 months.
Results: The determination of adequate bony resection margins with SPECT-CT yielded a sensitivity of 100% and a positive predictive value of 94.7%. Of all the bony resection margins, 97.4% were radiologically sufficiently ossified with the vascularized bone flap and showed no complications in the clinical course.
Conclusions: SPECT-CT could increase the probability of determining adequate bony resection margins.
Clinical relevance: SPECT-CT could have a beneficial clinical impact in the context of primary microvascular bony reconstruction in inflammatory jaw pathologies.
Keywords: Inflammatory jaw pathologies; Mandible reconstruction; Medication-related osteonecrosis of the jaw; Osteomyelitis; Osteoradionecrosis; SPECT-CT; Vascularized bone flaps.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: Ethical approval was granted by the Ethics Committee of the Medical Faculty of the RWTH Aachen, Germany (EK 24/037). This study was performed in accordance with the current version of the Declaration of Helsinki. Consent to participate: Not applicable. Consent to publish: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Doub JB et al (2024) Risk factors for infection recurrence after Surgical Resection of Advanced Stage Osteonecrosis of the Mandible. J Oral Maxillofac Surg 82(3):332–340 - PubMed
-
- Agarwal R et al (2022) Outcomes with culture-directed antibiotics following microvascular free tissue reconstruction for osteonecrosis of the jaw. Oral Oncol 130:105878 - PubMed
-
- Singh A et al (2019) Incidence, predictors and impact of positive bony margins in surgically treated T4 stage cancers of the oral cavity. Oral Oncol 90:8–12 - PubMed
-
- Assaf AT et al (2015) Intraindividual comparison of preoperative (99m)Tc-MDP SPECT/CT and intraoperative and histopathological findings in patients with bisphosphonate- or denosumab-related osteonecrosis of the jaw. J Craniomaxillofac Surg 43(8):1461–1469 - PubMed
-
- Strobel K et al (2012) Importance of SPECT/CT for resolving diseases of the jaw. Radiologe 52(7):638–645 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
