

Unusual Cutaneous Manifestations in a Patient with a History of Hepatitis B: A Case of Scleromyxedema and Literature Review
- PMID: 39872227
- PMCID: PMC11769843
- DOI: 10.2147/CCID.S492503
Unusual Cutaneous Manifestations in a Patient with a History of Hepatitis B: A Case of Scleromyxedema and Literature Review
Abstract
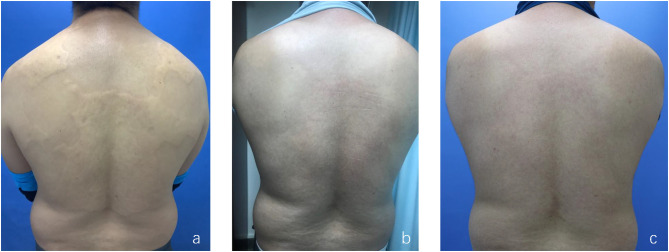
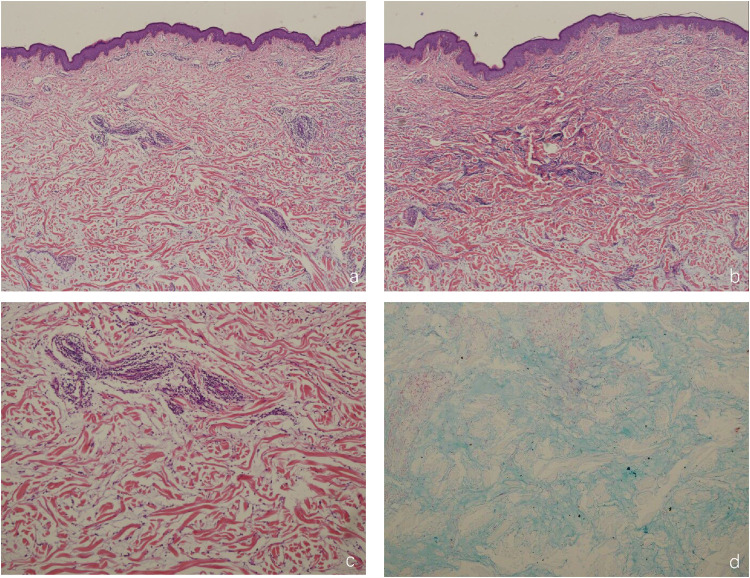
Scleromyxedema (SM) is a rare primary cutaneous mucinosis characterized by systemic papules and scleroderma-like manifestations, often associated with monoclonal gammopathy. We present the case of a 37-year-old male with SM who developed yellowish plaques on the neck and back over three years. Histopathological examination revealed mucin deposition, fibroblast proliferation, and fibrosis, supporting the diagnosis. Serum protein electrophoresis identified IgG-λ type paraproteinemia. Notably, the patient had a history of hepatitis B virus (HBV) infection, suggesting a potential association. Following eight weeks of oral triamcinolone acetonide therapy, the skin lesions improved significantly. Despite established diagnostic criteria for SM, its pathogenesis remains poorly understood. Chronic antigenic stimulation from circulating cytokines and viral infections, such as HBV, may contribute to disease development. This case highlights the potential link between chronic HBV infection and SM, emphasizing the need for further investigation into viral etiologies. SM differs clinically, histologically, and systemically from related disorders such as scleroderma and scleroedema, necessitating careful differentiation for appropriate management. The scarcity of epidemiological data and lack of standardized treatment guidelines for SM in China underscore the challenges clinicians face in diagnosing and managing this rare disease. This case reinforces the importance of multidisciplinary collaboration, particularly when co-infections such as HBV are present. Given the chronic, unpredictable course of SM and its potential systemic involvement, continuous follow-up and vigilant monitoring are essential to optimize patient outcomes.
Keywords: hepatitis B virus; mucin; paraglobulin; scleromyxedema.
© 2025 Gao et al.
Conflict of interest statement
The authors declare no conflicts of interest in this work.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
