

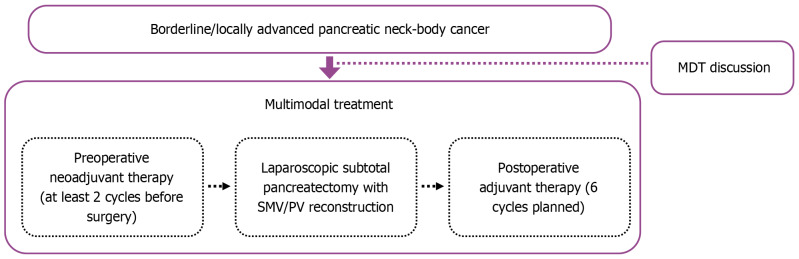
Multimodal treatment combining neoadjuvant therapy, laparoscopic subtotal distal pancreatectomy and adjuvant therapy for pancreatic neck-body cancer: Case series
- PMID: 39872794
- PMCID: PMC11757209
- DOI: 10.4240/wjgs.v17.i1.97897
Multimodal treatment combining neoadjuvant therapy, laparoscopic subtotal distal pancreatectomy and adjuvant therapy for pancreatic neck-body cancer: Case series
Abstract
Background: Pancreatic cancer involving the pancreas neck and body often invades the retroperitoneal vessels, making its radical resection challenging. Multimodal treatment strategies, including neoadjuvant therapy, surgery, and postoperative adjuvant therapy, are contributing to a paradigm shift in the treatment of pancreatic cancer. This strategy is also promising in the treatment of pancreatic neck-body cancer.
Aim: To evaluate the feasibility and effectiveness of a multimodal strategy for the treatment of borderline/locally advanced pancreatic neck-body cancer.
Methods: From January 2019 to December 2021, we reviewed the demographic characteristics, neoadjuvant and adjuvant treatment data, intraoperative and postoperative variables, and follow-up outcomes of patients who underwent multimodal treatment for pancreatic neck-body cancer in a prospectively collected database of our hospital. This investigation was reported in line with the Preferred Reporting of Case Series in Surgery criteria.
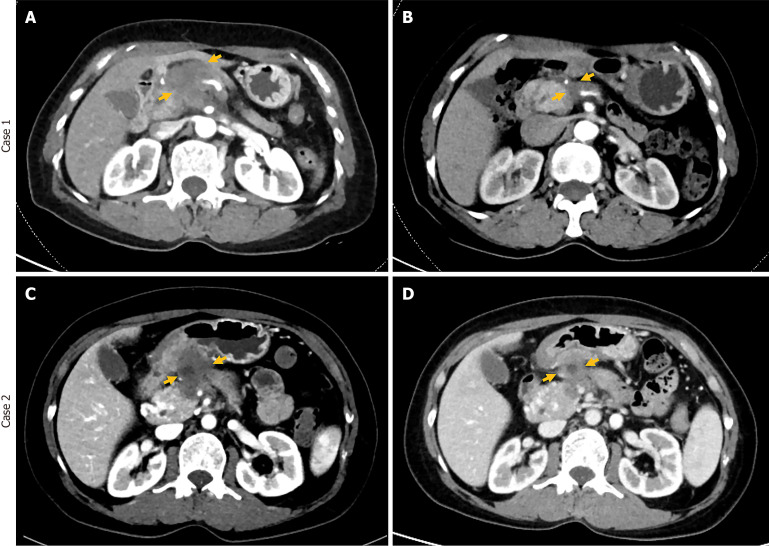
Results: A total of 11 patients with pancreatic neck-body cancer were included in this study, of whom 6 patients were borderline resectable and 5 were locally advanced. Through multidisciplinary team discussion, all patients received neoadjuvant therapy, of whom 8 (73%) patients achieved a partial response and 3 patients maintained stable disease. After multidisciplinary team reassessment, all patients underwent laparoscopic subtotal distal pancreatectomy and portal vein reconstruction and achieved R0 resection. Postoperatively, two patients (18%) developed ascites, and two patients (18%) developed pancreatic fistulae. The median length of stay of the patients was 11 days (range: 10-15 days). All patients received postoperative adjuvant therapy. During the follow-up, three patients experienced tumor recurrence, with a median disease-free survival time of 13.3 months and a median overall survival time of 20.5 months.
Conclusion: A multimodal treatment strategy combining neoadjuvant therapy, laparoscopic subtotal distal pancreatectomy, and adjuvant therapy is safe and feasible in patients with pancreatic neck-body cancer.
Keywords: Adjuvant therapy; Laparoscopic subtotal distal pancreatectomy; Multimodal treatment; Neoadjuvant therapy; Pancreatic neck-body cancer.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures


References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30. - PubMed
-
- Kleeff J, Korc M, Apte M, La Vecchia C, Johnson CD, Biankin AV, Neale RE, Tempero M, Tuveson DA, Hruban RH, Neoptolemos JP. Pancreatic cancer. Nat Rev Dis Primers. 2016;2:16022. - PubMed
-
- van Dam JL, Janssen QP, Besselink MG, Homs MYV, van Santvoort HC, van Tienhoven G, de Wilde RF, Wilmink JW, van Eijck CHJ, Groot Koerkamp B Dutch Pancreatic Cancer Group. Neoadjuvant therapy or upfront surgery for resectable and borderline resectable pancreatic cancer: A meta-analysis of randomised controlled trials. Eur J Cancer. 2022;160:140–149. - PubMed
-
- Imamura T, Yamamoto Y, Sugiura T, Okamura Y, Ito T, Ashida R, Ohgi K, Uesaka K. Reconsidering the Optimal Regional Lymph Node Station According to Tumor Location for Pancreatic Cancer. Ann Surg Oncol. 2021;28:1602–1611. - PubMed
LinkOut - more resources
Full Text Sources
