

Osteosarcoma tumor microenvironment: the key for the successful development of biologically relevant 3D in vitro models
- PMID: 39872973
- PMCID: PMC11756501
- DOI: 10.1007/s44164-022-00008-x
Osteosarcoma tumor microenvironment: the key for the successful development of biologically relevant 3D in vitro models
Abstract
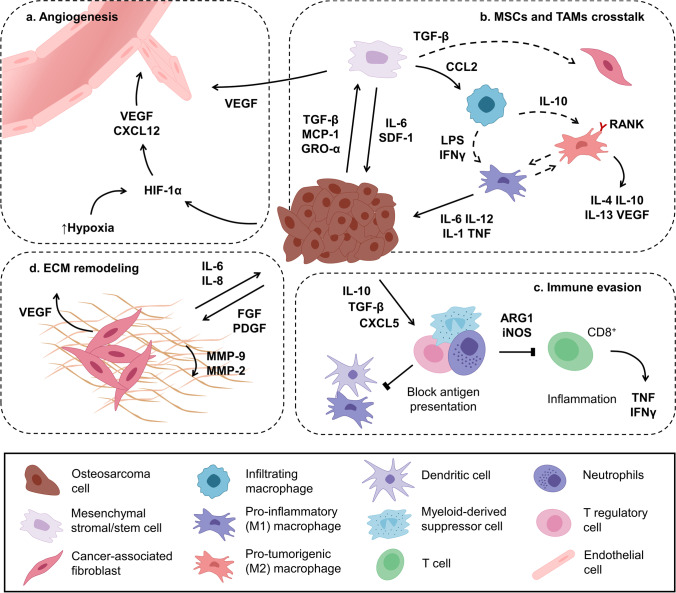
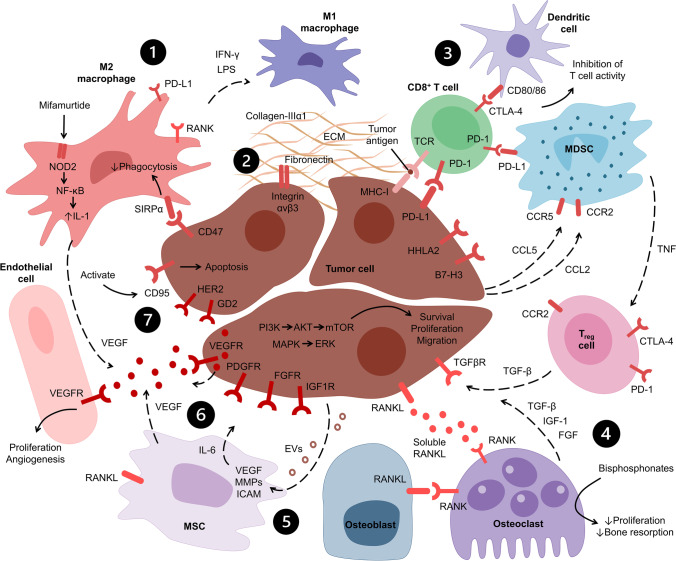
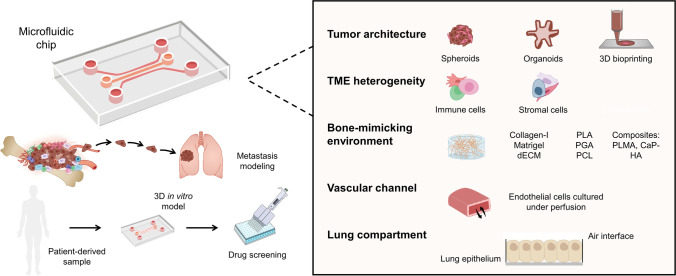
Osteosarcoma (OS) is the most common primary bone cancer in children and young adults. This type of cancer is characterized by a high mortality rate, especially for patients with resistant lung metastases. Given its low incidence, high genetic heterogeneity, the lack of effective targets, and poor availability of relevant in vitro and in vivo models to study the tumor progression and the metastatic cascade, the pathophysiology of OS is still poorly understood and the translation of novel drugs into the market has become stagnant. Due to the importance of the tumor microenvironment (TME) in the development of metastases and the growing interest in targeting TME-specific pathways for novel therapeutics in cancer, models that closely represent these interactions are crucial for a better understanding of cancer-related events. In OS research, most studies rely on oversimplified two-dimensional (2D) assays and complex animal models that do not faithfully recapitulate OS development and progression. In turn, three-dimensional (3D) models are able to mimic not only the physical 3D environment in which cancer cells grow but also involve interactions with the TME, including its extracellular matrix, and thus are promising tools for drug screening studies. In this review, the existing and innovative OS in vitro 3D models are highlighted, focusing on how the TME is crucial to develop effective platforms for OS tumor and metastasis modeling in a physiologically relevant context.
Keywords: 3D in vitro models; Metastasis; Microfluidics; Osteosarcoma; Tumor microenvironment.
© The Author(s), under exclusive licence to Springer Nature Switzerland AG 2022.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures

References
-
- Valery PC, Laversanne M, Bray F. Bone cancer incidence by morphological subtype: a global assessment. Cancer Causes Control. 2015;26:1127–39. 10.1007/s10552-015-0607-3. - PubMed
-
- Kansara M, Teng MW, Smyth MJ, Thomas DM. Translational biology of osteosarcoma. Nat Rev Cancer. 2014;14:722–35. 10.1038/nrc3838. - PubMed
-
- Casali PG, Bielack S, Abecassis N, Aro HT, Bauer S, Biagini R, et al. Bone sarcomas: ESMO–PaedCan–EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv79–95. 10.1093/annonc/mdy310. - PubMed
-
- Friebele JC, Peck J, Pan X, Abdel-Rasoul M, Mayerson JL. Osteosarcoma: a meta-analysis and review of the literature. Am J Orthop (Belle Mead NJ). 2015;44:547–53. - PubMed
Publication types
LinkOut - more resources
Full Text Sources