

Longitudinal impact of extended-hours hemodialysis with a liberalized diet on nutritional status and survival outcomes: findings from the LIBERTY cohort
- PMID: 39873816
- PMCID: PMC12125144
- DOI: 10.1007/s10157-024-02602-7
Longitudinal impact of extended-hours hemodialysis with a liberalized diet on nutritional status and survival outcomes: findings from the LIBERTY cohort
Abstract
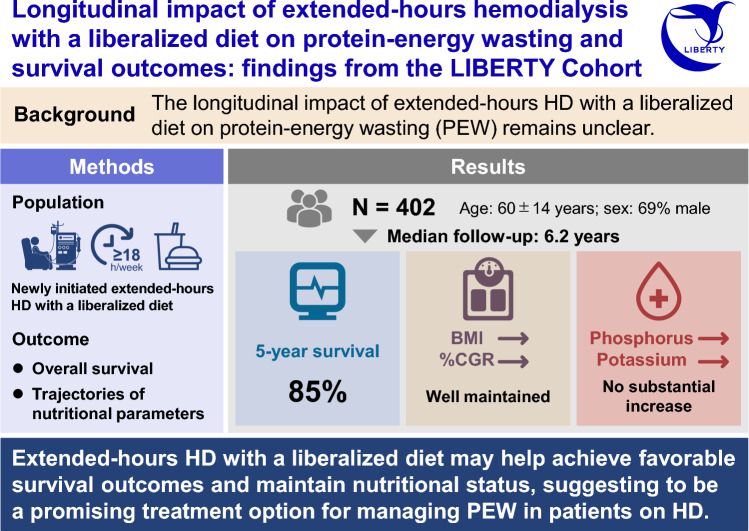
Background: Protein-energy wasting (PEW), a unique weight loss linked to nutritional and metabolic abnormalities, is common in patients undergoing hemodialysis (HD) and associated with adverse outcomes. This study investigated whether extended-hours HD combined with a liberalized diet could overcome PEW and improve survival.
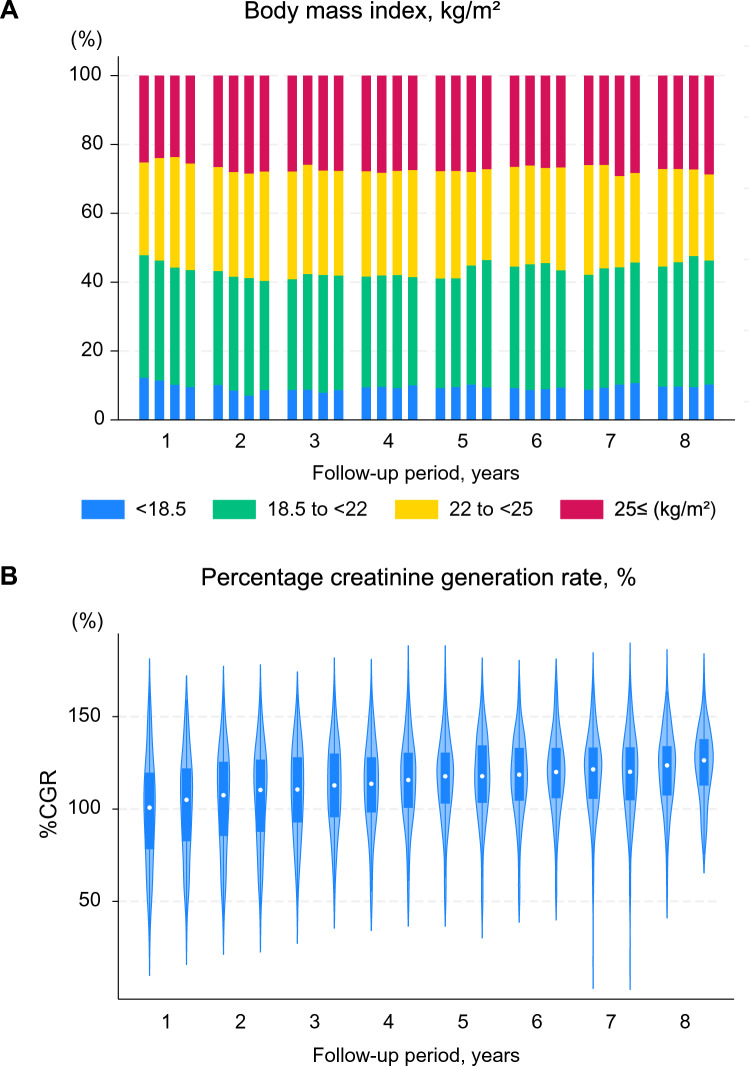
Methods: The body mass index (BMI) and survival outcomes in patients undergoing extended-hours HD were evaluated for up to 8 years using data from the LIBeralized diet Extended-houRs hemodialysis Therapy (LIBERTY) cohort. Extended-hours HD was defined as weekly dialysis length ≥ 18 h.
Results: The LIBERTY cohort included 402 patients who initiated extended-hours HD. An increase in the length and frequency of HD sessions was observed over time, with approximately 70% and 20% of patients undergoing extended-hours HD for > 21 h/week and > 3 sessions/week at 5 years, respectively. The BMI and percentage creatinine generation rate were maintained over time, with no substantial increase in the phosphorus and potassium levels. The estimated BMI initially increased, and thereafter plateaued over time in patients with a baseline BMI < 25 kg/m2, whereas it decreased gradually in patients with a baseline BMI ≥ 25 kg/m2 after several years from baseline. Ninety-one patients died, and 108 discontinued extended-hours HD during the median follow-up period of 6.2 years (interquartile range, 3.5-8.0), yielding a 5-year survival rate of 85%.
Conclusions: Extended-hours HD with a liberalized diet may help achieve favorable survival outcomes and maintain nutritional status. Thus, it is a promising treatment option for managing PEW in patients undergoing HD.
Keywords: Extended-hours hemodialysis; Liberalized diet; Longitudinal study; Protein-energy wasting.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interests: The authors have declared that no conflict of interest exists. Ethical approval: This study adhered to the tenets of the Declaration of Helsinki. The study protocol was approved by the ethics committee of the hospital. Informed consent: Written informed consent was obtained from the patients in the aforementioned prospective subset cohorts; however, the requirement for obtaining consent was waived for studies in which patients did not undergo invasive procedures and only anonymized data were obtained electronically.
Figures




References
-
- Jensen GL, Mirtallo J, Compher C, Dhaliwal R, Forbes A, Grijalba RF, et al. Adult starvation and disease-related malnutrition: a proposal for etiology-based diagnosis in the clinical practice setting from the international consensus guideline committee. J Parenter Enteral Nutr. 2010;34:156–9. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
