

The potential of lazertinib and amivantamab combination therapy as a treatment strategy for uncommon EGFR-mutated NSCLC
- PMID: 39874964
- PMCID: PMC11866483
- DOI: 10.1016/j.xcrm.2025.101929
The potential of lazertinib and amivantamab combination therapy as a treatment strategy for uncommon EGFR-mutated NSCLC
Abstract
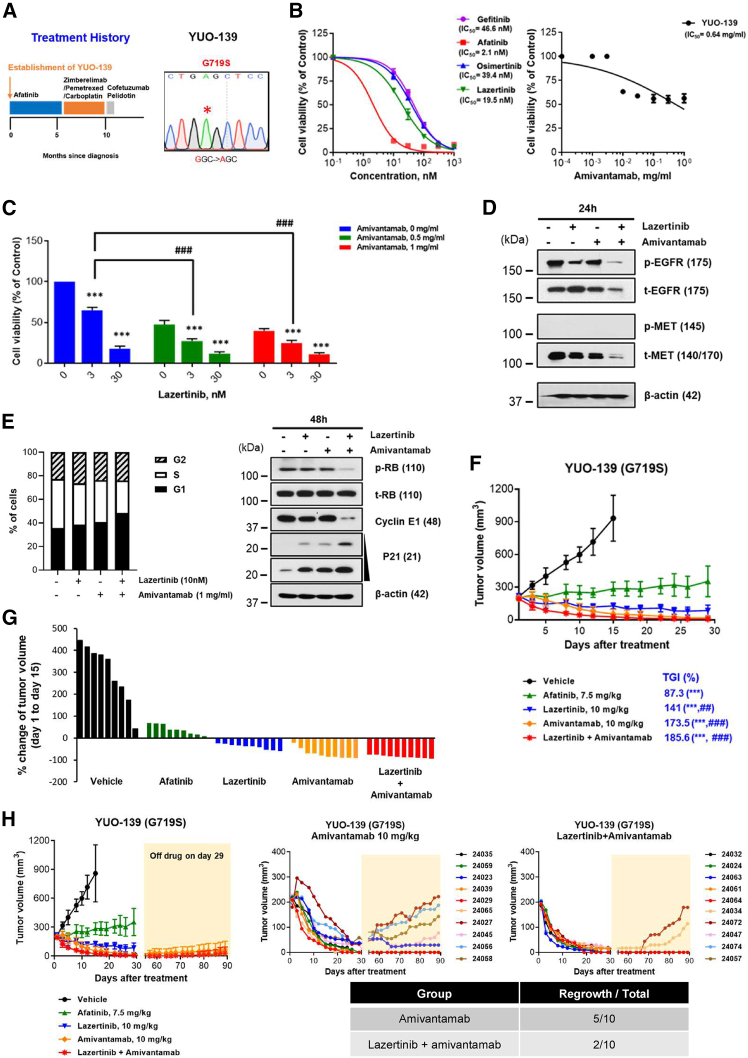
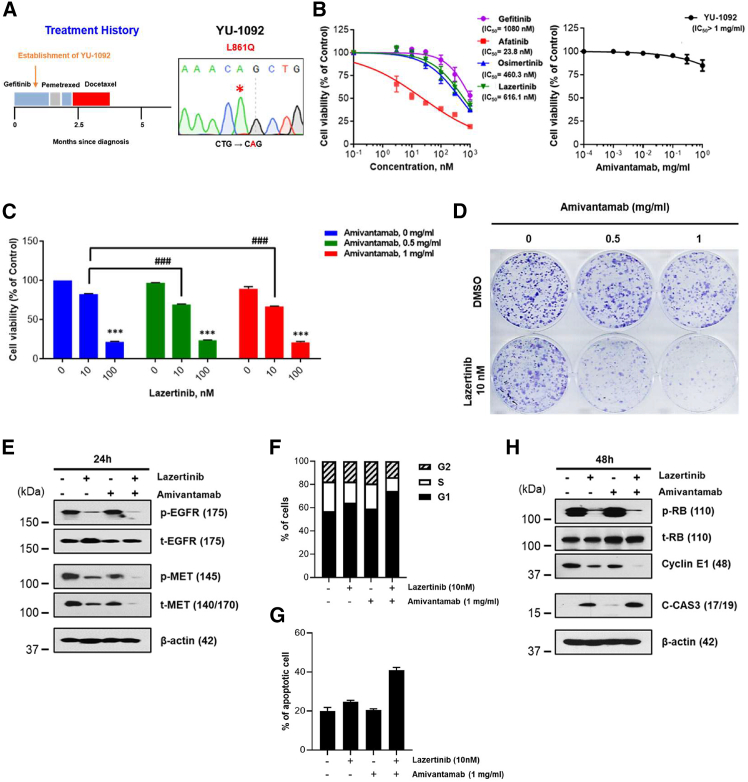
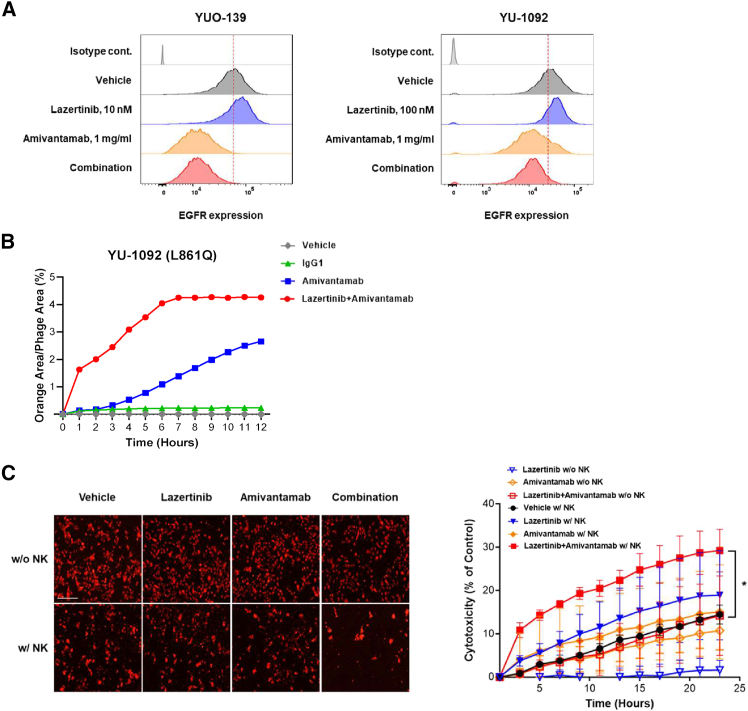
Uncommon epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer (NSCLC) pose therapeutic challenge due to limited response to EGFR tyrosine kinase inhibitors (TKIs). This study presents preclinical evidence and mechanistic insights into the combination of lazertinib, a third-generation EGFR-TKI; and amivantamab, an EGFR-MET bispecific antibody, for treating NSCLC with uncommon EGFR mutations. The lazertinib-amivantamab combination demonstrates significant antitumor activity in patient-derived models with uncommon EGFR mutations either before treatment or after progressing on EGFR-TKIs. Lazertinib enhances the inhibitory capacity of amivantamab by increasing its on-target expression. Notably, the combination surpasses afatinib, a first-line treatment for uncommon EGFR mutations in NSCLC, in terms of in vivo efficacy. Promising clinical activity is also observed in two case studies of patients treated with this combination (NCT04077463). Our findings highlight the potential of the lazertinib-amivantamab combination as a therapeutic strategy for uncommon EGFR mutations, an area of unmet medical need, and support further clinical investigation.
Keywords: EGFR-MET bispecific antibody; NSCLC; combination therapy; third-generation EGFR-TKI; uncommon EGFR-mutatation.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests B.C.C. declares the following competing interests: royalties from Champions Oncology, Crown Bioscience, Imagen, and PearlRiver Bio GmbH under licensing contracts for PDX, PDO, and PDC (not patent-related); research funding from GI Innovation, AstraZeneca, Champions Oncology, CJ Bioscience, Cyrus Therapeutics, Janssen, MSD, Dong-A ST, Yuhan, ImmuneOncia, Therapex Co., J INTS Bio, and Vertical Bio AG; consulting roles with BeiGene, Novartis, AstraZeneca, Boehringer Ingelheim, Roche, Bristol Myers Squibb (BMS), CJ Bioscience, Cyrus Therapeutics, Ono Pharmaceutical, Yuhan, Pfizer, Eli Lilly, Janssen, Takeda, MSD, Gilead, Amgen, Daiichi Sankyo, Regeneron, Sanofi, AnHeart Therapeutics, Seagen, Harpoon Therapeutics, GSK, and ArriVent; employment with Yonsei University Health System; advisory board memberships at KANAPH Therapeutics Inc., BridgeBio Therapeutics, Cyrus Therapeutics, Guardant Health, J INTS Bio, and Therapex Co., Ltd; invited speaker engagements for ASCO, AstraZeneca, Guardant, Roche, ESMO, IASLC, Korean Cancer Association, Korean Society of Medical Oncology, Korean Society of Thyroid-Head and Neck Surgery, Korean Cancer Study Group, Novartis, MSD, The Chinese Thoracic Oncology Society, Pfizer, and Zailab; stock holdings in TheraCanVac Inc., Gencurix Inc., BridgeBio Therapeutics, KANAPH Therapeutics Inc., Cyrus Therapeutics, Interpark Bio Convergence Corp., and J INTS Bio; and roles as founder of DAAN Biotherapeutics and board member of J INTS Bio. M.H.H. declares the following competing interests: honoraria from AstraZeneca, Amgen, BMS, MSD, Ono Pharmaceutical, Takeda, and Roche; consulting or advisory roles for AstraZeneca, BMS, MSD, Pfizer, Takeda, Roche, and Yuhan; investigator or co-investigator roles in clinical trials for AbbVie, AstraZeneca, BMS, IMPACT Therapeutics, Ignyta, Loxo Oncology, Merck Serono, MSD, Novartis, ORIC, Roche, Pfizer, and Yuhan; and research support from AstraZeneca, MSD, Novartis, and Yuhan.
Figures





References
-
- Travis W.D., Brambilla E., Nicholson A.G., Yatabe Y., Austin J.H.M., Beasley M.B., Chirieac L.R., Dacic S., Duhig E., Flieder D.B., et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015;10:1243–1260. - PubMed
-
- Wu Y.L., Cheng Y., Zhou X., Lee K.H., Nakagawa K., Niho S., Tsuji F., Linke R., Rosell R., Corral J., et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18:1454–1466. - PubMed
-
- Soria J.C., Ohe Y., Vansteenkiste J., Reungwetwattana T., Chewaskulyong B., Lee K.H., Dechaphunkul A., Imamura F., Nogami N., Kurata T., et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018;378:113–125. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
