

Pulmonary Morbidity in Congenital Diaphragmatic Hernia Survivors Treated at a Non-ECMO Center From 1998 to 2015: A Cross-Sectional Study
- PMID: 39876584
- PMCID: PMC11775427
- DOI: 10.1002/ppul.27468
Pulmonary Morbidity in Congenital Diaphragmatic Hernia Survivors Treated at a Non-ECMO Center From 1998 to 2015: A Cross-Sectional Study
Abstract
Introduction: A main feature of CDH is lung hypoplasia and the related presentation of pulmonary hypertension and cardiac dysfunction. Multiple factors influence pulmonary status after CDH: degree of hypoplasia, ventilator-induced injury, altered growth and development of pulmonary structures, reduced diaphragm function and chest wall abnormalities. The evolution of pulmonary sequela in this population is still unclear. We aimed to describe the pulmonary status of our population of CDH-survivors and evaluated on risk factors.
Methods: CDH-survivors (1998-2015) were included and performed lung function tests and chest X-rays.
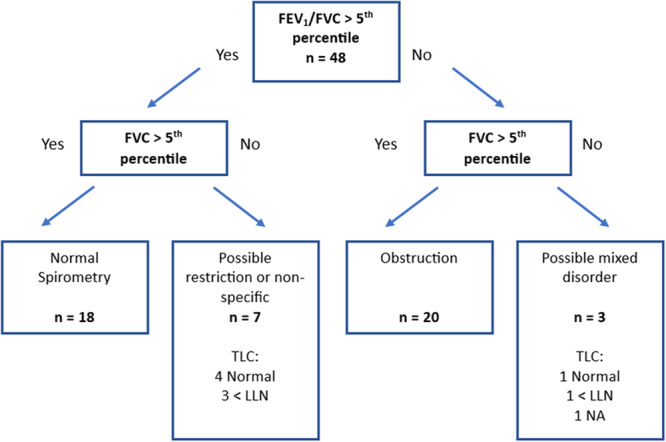
Results: Fifty-one (51/71, 71.8%) participated. Median age was 12.2 (5.5-21.4) years, 28 (54.9%) male, 42 (82.4%) had left-sided hernias, 10 (19.6%) needed patch-repair and median length of stay in hospital was 28.0 (IQR 18.5-61.6) days in Table 1. Spirometry including bronchodilator response (BDR)-test, body plethysmography, and diffusion capacity, were available for 48, 42, and 40 participants. The mean (SD) z-score for FEV1 and FVC was -0.26 (1.70) and -0.28 (1.70). Twenty-one (43.8%) had obstructive patterns and six had positive BDR. TLC mean (SD) z-score was -0.18 (1.10). Four showed restricted/mixed patterns and 13 showed signs of hyperinflation. Increased RV/TLC-ratio and reduced FEV1 was associated with longer time on mechanical ventilation. Diffusion capacity was decreased in three cases. Chest X-ray revealed hernia recurrence (13.9%) and scoliosis (38.9%).
Conclusion: Mild obstructive impairment and hyperinflation was frequent in our CDH cohort and only a small subset of restrictive disorders were identified. We advocate follow-up by a specialized multidisciplinary team through childhood and into adulthood.
© 2025 The Author(s). Pediatric Pulmonology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Cardiopulmonary exercise performance is reduced in congenital diaphragmatic hernia survivors.Pediatr Pulmonol. 2016 Dec;51(12):1320-1329. doi: 10.1002/ppul.23481. Epub 2016 May 26. Pediatr Pulmonol. 2016. PMID: 27228382
-
Therapy at 30 days of life predicts lung function at 6 to 12 months in infants with congenital diaphragmatic hernia.Pediatr Pulmonol. 2020 Jun;55(6):1456-1467. doi: 10.1002/ppul.24736. Epub 2020 Mar 19. Pediatr Pulmonol. 2020. PMID: 32191392
-
Cardiopulmonary anatomy and function in long-term survivors of mild to moderate congenital diaphragmatic hernia.J Pediatr Surg. 2004 Apr;39(4):526-31. doi: 10.1016/j.jpedsurg.2003.12.006. J Pediatr Surg. 2004. PMID: 15065021
-
The long-term follow-up of patients with a congenital diaphragmatic hernia: a broad spectrum of morbidity.Pediatr Surg Int. 2009 Jan;25(1):1-17. doi: 10.1007/s00383-008-2257-y. Epub 2008 Oct 8. Pediatr Surg Int. 2009. PMID: 18841373 Review.
-
Congenital diaphragmatic hernia-associated pulmonary hypertension.Semin Pediatr Surg. 2024 Aug;33(4):151437. doi: 10.1016/j.sempedsurg.2024.151437. Epub 2024 Jul 2. Semin Pediatr Surg. 2024. PMID: 39018718 Review.
References
-
- Greer J. J., “Current Concepts on the Pathogenesis and Etiology of Congenital Diaphragmatic Hernia,” Respiratory Physiology & Neurobiology 189, no. 2 (2013): 232–240. - PubMed
-
- Thibeault D. W. and Haney B., “Lung Volume, Pulmonary Vasculature, and Factors Affecting Survival in Congenital Diaphragmatic Hernia,” Pediatrics 101, no. 2 (1998): 289–295. - PubMed
-
- Jani J., Nicolaides K. H., Keller R. L., et al., “Observed to Expected Lung Area to Head Circumference Ratio in the Prediction of Survival in Fetuses With Isolated Diaphragmatic Hernia,” Ultrasound in Obstetrics & Gynecology 30, no. 1 (2007): 67–71. - PubMed
-
- Muratore C. S., Kharasch V., Lund D. P., et al., “Pulmonary Morbidity in 100 Survivors of Congenital Diaphragmatic Hernia Monitored in a Multidisciplinary Clinic,” Journal of Pediatric Surgery 36, no. 1 (2001): 133–140. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
