

Linear IgA bullous dermatosis-a fifty year experience of Warsaw Center of bullous diseases
- PMID: 39877369
- PMCID: PMC11772161
- DOI: 10.3389/fimmu.2024.1478318
Linear IgA bullous dermatosis-a fifty year experience of Warsaw Center of bullous diseases
Abstract
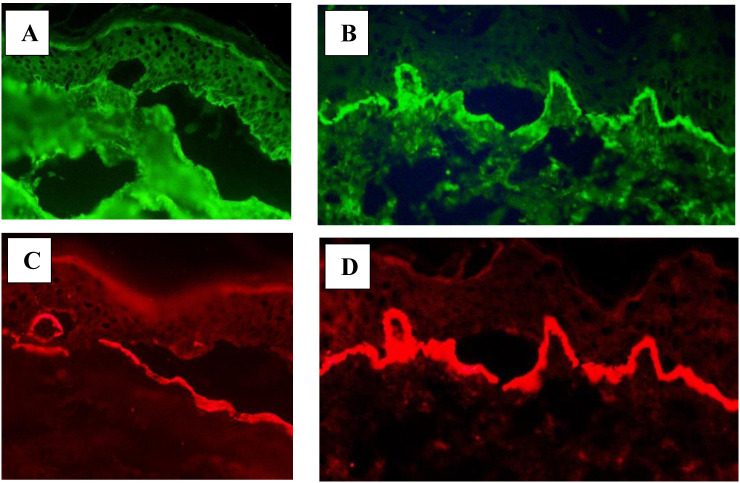
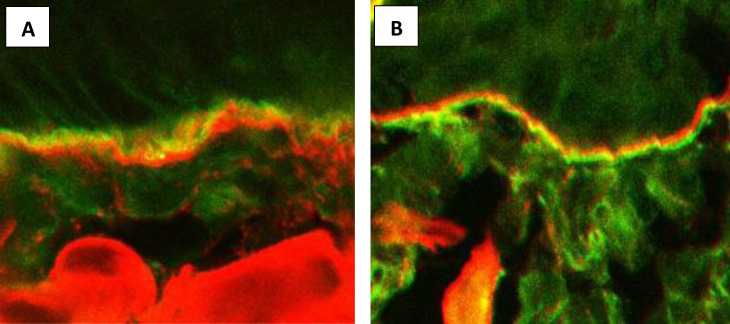
Linear IgA bullous dermatosis (LABD) is a rare subepidermal blistering disorder characterized by the presence of linear IgA deposits at the basement membrane zone (BMZ) by direct immunofluorescence (DIF). This entity was first described by Chorzelski and Jablonska from Warsaw Center of Bullous Diseases, Poland. The disease affects children and adults, whereby they differ in terms of clinical picture and course. Among polish patients with LABD mucous membrane involvement was exceptional, although, we reported a case presenting severe scarring of esophagus and conjunctivae with circulating IgG and IgA antibodies to LAD-1 antigen. Severe mucosal involvement was also observed in IgA-epidermolysis bullosa acquisita (EBA). Immunologically, LABD is characterized by circulating IgA antibodies directed to several epitopes of antigen BP180: LAD-1, 97kD, NC16A. Other BMZ antigens, like BP230, laminin 332, type VII collagen or p200 may be affected. We as a first published a case of anti-p200kD pemphigoid mediated by IgA. Our immunoelectron microscopic studies showed that the epitopes recognized by LABD sera are ultrastructurally localized in the lamina lucida. The antigenic heterogeneity, low titer of IgA antibodies and the lack of commercially available tests for some antigens (LAD-1, p200kD) makes the diagnosis challenging in many cases. It is under debate whether these cases are the subtypes of LABD or they represent a separate entities (IgA-p200 pemphigoid, IgA-MMP or IgA-EBA). Since, they differ in terms of clinical course, mucosal involvement, coexisting disorders, response to the treatment and prognosis, their differentiation is mandatory. In the literature there are many cases with undetectable circulating IgA antibodies in whom LABD was recognized based on DIF only. To avoid misdiagnosis, more sophisticated methods should be used, like direct immunoeletron microscopy (IEM), which is a time-consuming technique. The alternative for IEM may be: a) analysis of the BMZ serration pattern, b) immunofluorescence mapping of blister, c) direct salt split (patient's) skin, d) fluorescence overlay antigen mapping by laser scanning confocal microscopy. The two latter methods were established by the authors years ago and they allowed precise diagnosis (i.e., differentiation LABD from IgA-EBA), initiation of proper therapy and assessment of prognosis in many cases mediated by IgA.
Keywords: IgA epidermolysis bullosa acquisita; direct immunofluorescence; direct split skin; fluorescence overlay antigen mapping by laser scanning confocal microscopy; linear IgA bullous dermatosis.
Copyright © 2025 Kowalewski and Wozniak.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Fluorescence overlay antigen mapping using laser scanning confocal microscopy differentiates linear IgA bullous dermatosis from epidermolysis bullosa acquisita mediated by IgA.Br J Dermatol. 2013 Mar;168(3):634-8. doi: 10.1111/bjd.12017. Br J Dermatol. 2013. PMID: 22924407
-
Linear IgA bullous dermatosis in a latin adolescent treated with cyclosporine and prednisone.Bol Med Hosp Infant Mex. 2024;81(5):305-310. doi: 10.24875/BMHIM.24000043. Bol Med Hosp Infant Mex. 2024. PMID: 39378410 English.
-
A Case of Possible Concurrence of Dermatitis Herpetiformis and Linear Immunoglobulin A / Immunoglobulin G Bullous Dermatosis.Acta Dermatovenerol Croat. 2021 Jul;29(2):116-117. Acta Dermatovenerol Croat. 2021. PMID: 34477081
-
Brunsting-Perry pemphigoid: a systematic review.Int J Dermatol. 2022 Nov;61(11):1353-1358. doi: 10.1111/ijd.16045. Epub 2022 Jan 20. Int J Dermatol. 2022. PMID: 35049061
-
Updates in the Diagnosis and Management of Linear IgA Disease: A Systematic Review.Medicina (Kaunas). 2021 Aug 12;57(8):818. doi: 10.3390/medicina57080818. Medicina (Kaunas). 2021. PMID: 34441024 Free PMC article.
References
-
- Chorzelski TP, Jablonska S, Beutner E, Dale W. Immunopathology of the skin. Ed 3 Vol. 1985. Beutner E, Chorzelski TP, Kumar V, editors. New York: Wiley; (1985) p. p407–420.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous