

A head-to-head comparison of the adult EQ-5D-5L and youth EQ-5D-Y-5L in adolescents with idiopathic scoliosis
- PMID: 39878911
- PMCID: PMC11780234
- DOI: 10.1186/s41687-025-00842-z
A head-to-head comparison of the adult EQ-5D-5L and youth EQ-5D-Y-5L in adolescents with idiopathic scoliosis
Abstract
Background: Multiple diseases, such as Adolescent Idiopathic Scoliosis (AIS), present at adolescent age and the impact on quality of life (QoL) prolongs into adulthood. For the EQ-5D, a commonly used instrument to measure QoL, the current guideline is ambiguous whether the youth or adult version is to be preferred at adolescent age. To assess which is most suitable, this study tested for equivalence along predefined criteria of the youth (EQ-5D-5L) and adult (EQ-5D-Y-5L) version in an adolescent population receiving bracing therapy for AIS.
Methodology: 107 adolescents were recruited from 4 scoliosis centers in the Netherlands between March 2022 and January 2023; they completed both EQ-5D's and the SRS-22r (scoliosis-specific questionnaire). The following criteria were evaluated using the individual and sum of domains (level-sum-score (LSS)). Our primary criterion for non-equivalence of the EQ-5D's was less than excellent (≤ 0.9) intra-individual agreement using Intraclass Correlation Coefficient (ICC) analysis for LSS and weighted (quadratic) kappa for domains. Secondary criteria were differences in ceiling using McNemar test; a different number of quantified hypotheses for construct validity achieved using the SRS-22r as comparator; differences in test-retest reliability by comparing ICC/kappa values using a Z-test.
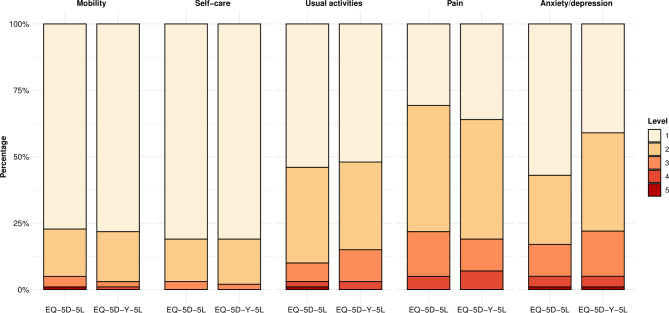
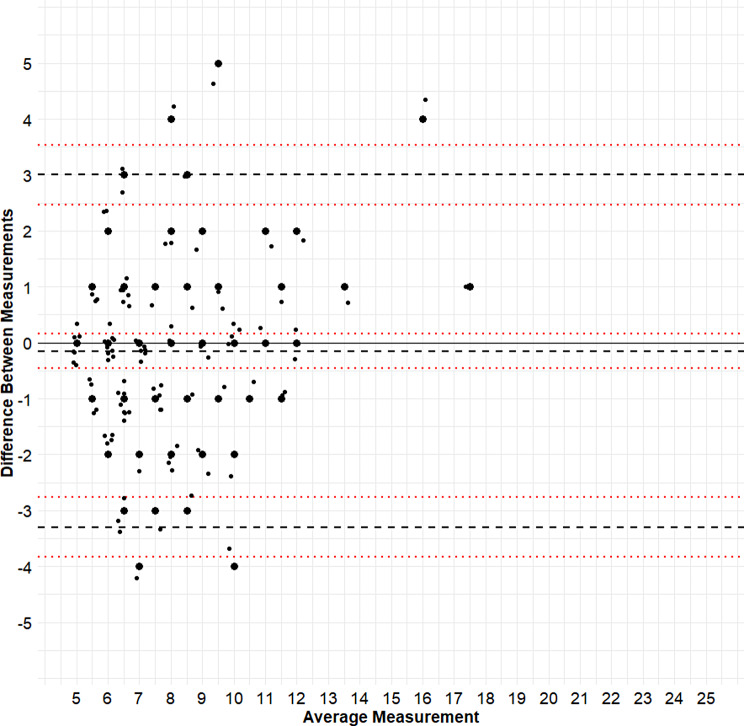
Results: Adolescents had a mean age of 14 years (range 12-18), and 78% were female. Ceiling was mostly comparable between EQ-5D's, ranging from 78 to 81% for mobility and self-care, 52-54% for usual activities, and 31-36% for pain/discomfort. The EQ-5D-5L showed more ceiling (57%) compared to the EQ-5D-Y-5L (41%) on anxiety/depression (p = 0.006). Agreement between the EQ-5D's did not meet our criterion for the LSS (ICC 0.79 (95% confidence interval 0.70-0.85)), and decreased further at the domain-level. Both EQ-5D's achieved 5/7 validity hypotheses. Test-retest reliability was slightly better for EQ-5D-5L LSS (ICC 0.76 (0.64-0.84)) compared to EQ-5D-Y-5L LSS (ICC 0.69 (0.55-0.79)), although this was statistically insignificant (p = 0.284). This pattern was similar for most domains.
Conclusions: The EQ-5D versions showed insufficient agreement, and cannot be considered fully equivalent. While they were similar in terms of validity and test-retest reliability, differences in score distribution were present. Taken together, we advise using the EQ-5D-5L to monitor the QoL in adolescent patients with AIS, as it avoids switching instruments and thus data discontinuities. Future studies should verify these findings in different patient groups and the general population.
Keywords: Adolescent idiopathic scoliosis; Adult; Children; Clinical registries; EQ-5D-5L; EQ-5D-Y-5L; Equivalence; Longitudinal; Quality of life; Youth.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This study was approved by the Medical Ethical Review Board from University Medical Center Groningen (reference number 202100536); study-site specific ethical approval of each participating center was also obtained. Consent to participate: Eligible patients (and their parent/guardian) received oral and standardized written information on the study, and participants were required to provide consent conform Dutch law. Adolescents aged 12 to 16 give are required to provide consent independently in addition to their parents or guardian. From 17 and older, adolescents sign themselves (if deemed capable). Although not required by Dutch law, two versions of written information were provided. The first (standard) was tailored towards adults including adolescents aged > 16, while the second (additional) was tailored towards children aged 12 to 16. The latter used child-friendly language and terminology. At each site, consent was obtained by researchers and orthopedic surgeons with knowledge of the patient population and the study. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Psychometric performance of proxy-reported EQ-5D youth version 5-level (EQ-5D-Y-5L) in comparison with three-level (EQ-5D-Y-3L) in children and adolescents with scoliosis.Eur J Health Econ. 2022 Nov;23(8):1383-1395. doi: 10.1007/s10198-022-01435-z. Epub 2022 Feb 4. Eur J Health Econ. 2022. PMID: 35122171
-
Psychometric validation of the EuroQoL 5-Dimension 5-Level (EQ-5D-5L) in Chinese patients with adolescent idiopathic scoliosis.Scoliosis Spinal Disord. 2016 Aug 4;11:19. doi: 10.1186/s13013-016-0083-x. eCollection 2016. Scoliosis Spinal Disord. 2016. PMID: 27525314 Free PMC article.
-
Mapping the SRS-22r questionnaire onto the EQ-5D-5L utility score in patients with adolescent idiopathic scoliosis.PLoS One. 2017 Apr 17;12(4):e0175847. doi: 10.1371/journal.pone.0175847. eCollection 2017. PLoS One. 2017. PMID: 28414745 Free PMC article.
-
Head-to-Head Comparisons of the Distributional Characteristics and Measurement Properties of the 3-Level and 5-Level Versions of the EQ-5D-Y: A Systematic Review.Value Health. 2025 Apr 15:S1098-3015(25)02303-4. doi: 10.1016/j.jval.2025.03.020. Online ahead of print. Value Health. 2025. PMID: 40246069 Review.
-
Measurement Properties of the EQ-5D Instruments in Children and Adolescents: A Systematic Review.Appl Health Econ Health Policy. 2025 Apr 19. doi: 10.1007/s40258-025-00953-0. Online ahead of print. Appl Health Econ Health Policy. 2025. PMID: 40252155
References
-
- Brooks R (1996) EuroQol: the current state of play. Health Policy 37(1):53–72. 10.1016/0168-8510(96)00822-6 - PubMed
-
- Wong CKH, Cheung PWH, Luo N, Cheung JPY (2019) A head-to-head comparison of five-level (EQ-5D-5L-Y) and three-level EQ-5D-Y questionnaires in paediatric patients. Eur J Health Econ 20(5):647–656 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
