

Contribution of Blood Biomarkers to Multiple Sclerosis Diagnosis
- PMID: 39879564
- PMCID: PMC11781269
- DOI: 10.1212/NXI.0000000000200370
Contribution of Blood Biomarkers to Multiple Sclerosis Diagnosis
Abstract
Background and objectives: Invasive procedures may delay the diagnostic process in multiple sclerosis (MS). We investigated the added value of serum neurofilament light chain (sNfL), glial fibrillary acidic protein (sGFAP), chitinase-3-like 1 (sCHI3L1), and the immune responses to the Epstein-Barr virus-encoded nuclear antigen 1 to current MS diagnostic criteria.
Methods: In this multicentric study, we selected patients from 2 prospective cohorts presenting a clinically isolated syndrome (CIS). Patients were classified as (1) not presenting dissemination in space (DIS) nor dissemination in time (DIT) (noDIS and noDIT); (2) presenting DIS without DIT (DIS and noDIT); and (3) presenting both (DIS and DIT), which were used as a reference. sNfL, sGFAP, and sCHI3L1 levels were measured with single-molecule array immunoassays and EBNA1-specific IgG levels with ELISA. Biomarker levels were compared between groups using linear regression models. Receiver operating characteristic curve analyses and Youden Index were used to determine cutoff values associated with MS diagnosis during follow-up.
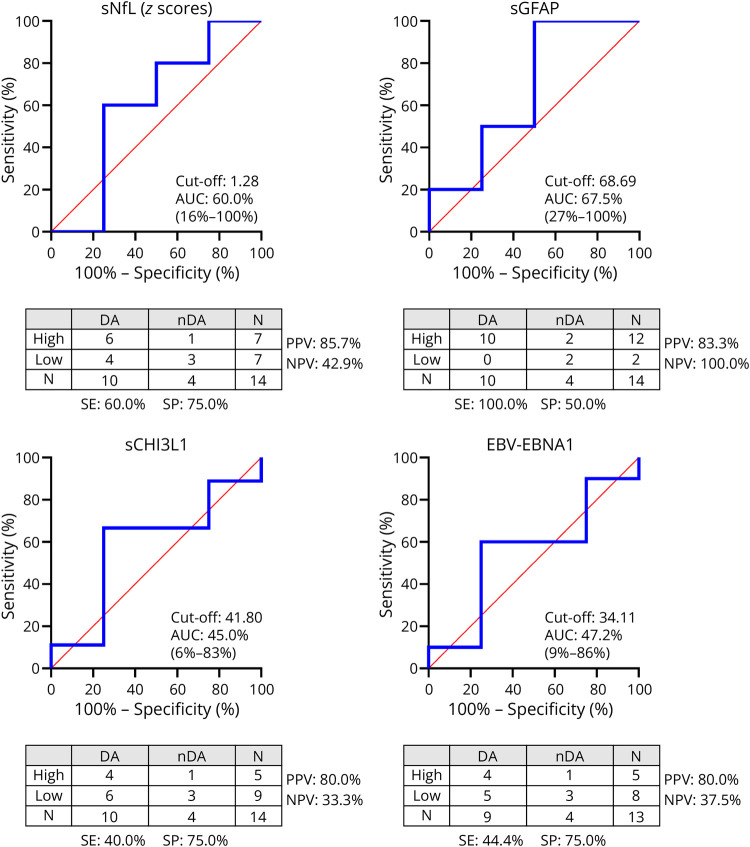
Results: We included 181 patients (66.3% females, mean [SD] age of 35.0 [9.7] years). At baseline, 25 (13.8%) were classified as noDIS and noDIT, 62 (34.3%) as DIS and noDIT, and 94 (51.9%) as DIS and DIT. Only sNfL Z-scores discriminated between groups (DIS and DIT vs DIS and noDIT [p = 0.002], DIS and DIT vs noDIS and noDIT [p < 0.001], and DIS and noDIT vs noDIS and noDIT [p = 0.026]). In noDIS and noDIT patients (median interquartile range [IQR] follow-up of 8.1 [5.0-11.7] years), high sNfL Z-scores best predicted MS diagnosis (specificity [SP] and 95% CI of 93.3% [68.1-99.8] and positive predictive value [PPV] of 87.5% [47.3-99.7]). Among DIS and noDIT patients (median [IQR] follow-up of 6.8 [4.0-9.1] years), high sNfL Z-scores best predicted MS diagnosis (SP of 80% [28.4-99.5] and PPV of 97.3% [85.8-99.9]) without considering oligoclonal band (OB) status. In the subset of patients of this group with negative OBs, a combination of high sNfL Z-scores and sGFAP levels predicted MS diagnosis (SP of 100% [39.8-100] and PPV of 100% [54.1-100]).
Discussion: These results suggest that sNfL and sGFAP may be incorporated in particular scenarios to diagnose MS in patients with CIS not fulfilling current diagnostic criteria.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous