

Association of Year-to-Year Lipid Variability With Risk of Cognitive Decline and Dementia in Community-Dwelling Older Adults
- PMID: 39879572
- PMCID: PMC11774555
- DOI: 10.1212/WNL.0000000000210247
Association of Year-to-Year Lipid Variability With Risk of Cognitive Decline and Dementia in Community-Dwelling Older Adults
Abstract
Background and objectives: Lipid metabolism in older adults is affected by various factors including biological aging, functional decline, reduced physiologic reserve, and nutrient intake. The dysregulation of lipid metabolism could adversely affect brain health. This study investigated the association between year-to-year intraindividual lipid variability and subsequent risk of cognitive decline and dementia in community-dwelling older adults.
Methods: ASPirin in Reducing Events in the Elderly (ASPREE) was a randomized trial of aspirin, involving 19,114 participants aged 65 years and older from Australia and the United States who were free of dementia and major cognitive impairment. ASPREE-eXTension is the post-trial observational follow-up of participants, currently to a maximum of 11 years. This post hoc analysis included participants who had lipid levels measured at baseline and in years 1, 2, and 3. Year-to-year variability in total cholesterol (TC), low-density lipoprotein cholesterol (LDL-c), high-density lipoprotein cholesterol (HDL-c), and triglycerides over the first 3 years was quantified using variability independent of the mean. Individuals who initiated or discontinued lipid-lowering therapy during this period were excluded. Multivariable Cox proportional hazards regression was used to analyze associations with incident dementia, adjudicated by expert panels, and cognitive impairment with no dementia (CIND) confirmed by a battery of cognitive tests, occurring after year 3. A linear mixed model was used for assessing the association with changes in 4 cognitive function domains, including global, memory, processing speed, verbal fluency, and a composite score from baseline to the end of follow-up.
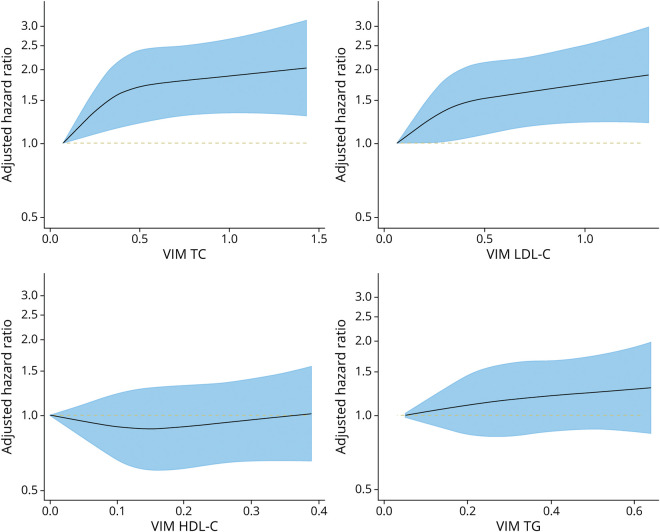
Results: The analysis included 9,846 individuals (median [interquartile range] age: 73.9 [71.7-77.3] years, 54.9% female). 509 incident dementia and 1,760 CIND events were recorded over a median follow-up of 5.8 and 5.4 years after variability assessment. The hazard ratios (95% CI) comparing the highest and lowest quartiles of TC and LDL-c variability were 1.60 (1.23-2.08) and 1.48 (1.15-1.91) for dementia and 1.23 (1.08-1.41) and 1.27 (1.11-1.46) for CIND. Higher TC and LDL-c variability was also associated with a faster decline in global cognition, episodic memory, psychomotor speed, and the composite score (all p < 0.001). No strong evidence was found for an association of HDL-c and triglyceride variability with dementia and cognitive change.
Discussion: Tracking variability of TC and LDL-c may serve as a novel biomarker of incident dementia and cognitive decline in older adults.
Conflict of interest statement
Z. Zhou is supported by a 2022 Postdoctoral Fellowship (106578) from the National Heart Foundation of Australia to lead this work. S. Zoungas has received NHMRC and Australian Heart Foundation research funding as the principal investigator of the STAREE trial and has received payment to the institution (Monash University) from Eli Lilly Australia, Boehringer-Ingelheim, Merck Sharp & Dohme Australia, AstraZeneca, Novo Nordisk, Sanofi, and Servier for consultancy work outside the submitted work. T.T.-J. Chong has received honoraria for lectures from Roche. R.C. Shah is a member of the steering committee of the PREVENTABLE clinical trial. M. Nelson reported receiving speaker fees from Medtronic, and honoraria from Sanofi and Amgen, as well as from Bayer for materials in ASPREE. A.M. Tonkin reported receiving research support or honoraria from Amgen, Merck, Novartis and Pfizer, as well as materials in the ASPREE trial from Bayer. C. Moran, A.M. Murray, C. Magnussen, K.M. Sheets, C. Zhu, S. Talic, M.E. Ernst, S.G. Orchard, J.J. McNeil, R. Wolfe, R.L. Woods, J.T. Neumann, P. Qiu, and J. Ryan reported no relevant disclosures. Go to
Figures



References
-
- Kivipelto M, Helkala EL, Laakso MP, et al. . Apolipoprotein E epsilon4 allele, elevated midlife total cholesterol level, and high midlife systolic blood pressure are independent risk factors for late-life Alzheimer disease. Ann Intern Med. 2002;137(3):149-155. doi:10.7326/0003-4819-137-3-200208060-00006 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical