

Oral Regimens for Rifampin-Resistant, Fluoroquinolone-Susceptible Tuberculosis
- PMID: 39879593
- PMCID: PMC7617355
- DOI: 10.1056/NEJMoa2400327
Oral Regimens for Rifampin-Resistant, Fluoroquinolone-Susceptible Tuberculosis
Abstract
Background: For decades, poor treatment options and low-quality evidence plagued care for patients with rifampin-resistant tuberculosis. The advent of new drugs to treat tuberculosis and enhanced funding now permit randomized, controlled trials of shortened-duration, all-oral treatments for rifampin-resistant tuberculosis.
Methods: We conducted a phase 3, multinational, open-label, randomized, controlled noninferiority trial to compare standard therapy for treatment of fluoroquinolone-susceptible, rifampin-resistant tuberculosis with five 9-month oral regimens that included various combinations of bedaquiline (B), delamanid (D), linezolid (L), levofloxacin (Lfx) or moxifloxacin (M), clofazimine (C), and pyrazinamide (Z). Participants were randomly assigned (with the use of Bayesian response-adaptive randomization) to receive one of five combinations or standard therapy. The primary end point was a favorable outcome at week 73, defined by two negative sputum culture results or favorable bacteriologic, clinical, and radiologic evolution. The noninferiority margin was -12 percentage points.
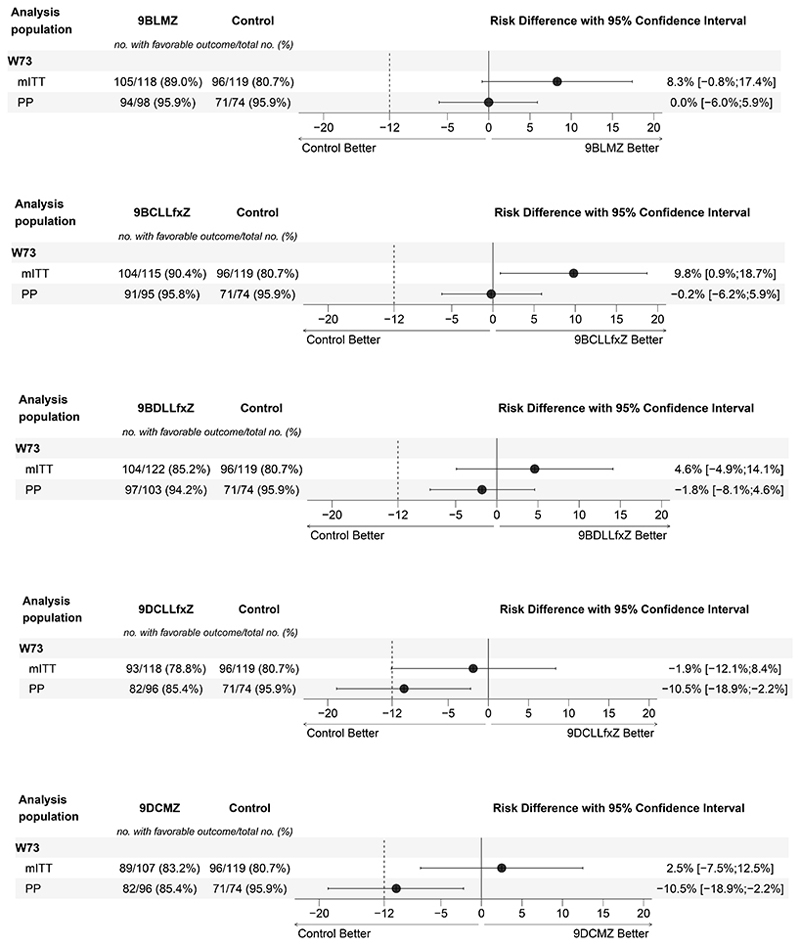
Results: Among the 754 participants who underwent randomization, 699 were included in the modified intention-to-treat analysis, and 562 in the per-protocol analysis. In the modified intention-to-treat analysis, 80.7% of the patients in the standard-therapy group had favorable outcomes. The risk difference between standard therapy and each of the four new regimens that were found to be noninferior in the modified intention-to-treat population was as follows: BCLLfxZ, 9.8 percentage points (95% confidence interval [CI], 0.9 to 18.7); BLMZ, 8.3 percentage points (95% CI, -0.8 to 17.4); BDLLfxZ, 4.6 percentage points (95% CI, -4.9 to 14.1); and DCMZ, 2.5 percentage points (95% CI, -7.5 to 12.5). Differences were similar in the per-protocol population, with the exception of DCMZ, which was not noninferior in that population. The proportion of participants with grade 3 or higher adverse events was similar across the regimens. Grade 3 or higher hepatotoxic events occurred in 11.7% of participants overall and in 7.1% of those receiving standard therapy.
Conclusions: Consistent results across all the analyses support the noninferior efficacy of three all-oral shortened regimens for the treatment of rifampin-resistant tuberculosis. (Funded by Unitaid and others; endTB ClinicalTrials.gov number, NCT02754765.).
Copyright © 2025 Massachusetts Medical Society.
Figures

References
-
- WHO. Global tuberculosis report 2023. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 30 IGO Published online 2023.
-
- WHO. WHO Treatment guidelines for drug-resistant tuberculosis – 2016 update. WHO; Geneva Switz: 2016. WHO/HTM/TB/201604. Published online 2016. - PubMed
-
- Goodall RL, Meredith SK, Nunn AJ, et al. Evaluation of two short standardised regimens for the treatment of rifampicin-resistant tuberculosis (STREAM stage 2): an open-label, multicentre, randomised, non-inferiority trial. The Lancet. 2022;400(10366):1858–1868. doi: 10.1016/S0140-6736(22)02078-5. - DOI - PMC - PubMed