

A functional cardiac patch promotes cardiac repair by modulating the CCR2- cardiac-resident macrophage niche and their cell crosstalk
- PMID: 39879993
- PMCID: PMC11866506
- DOI: 10.1016/j.xcrm.2025.101932
A functional cardiac patch promotes cardiac repair by modulating the CCR2- cardiac-resident macrophage niche and their cell crosstalk
Abstract
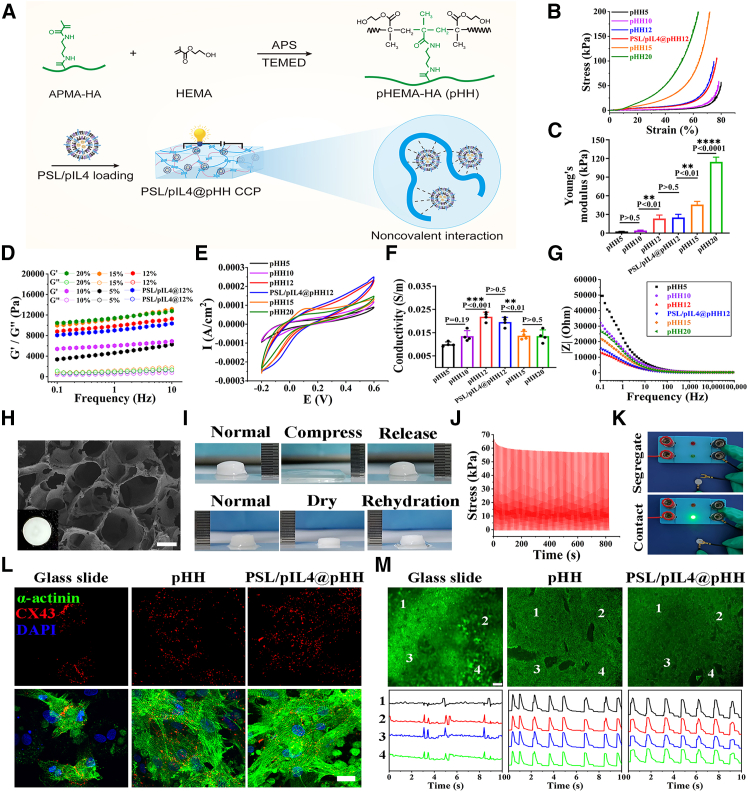
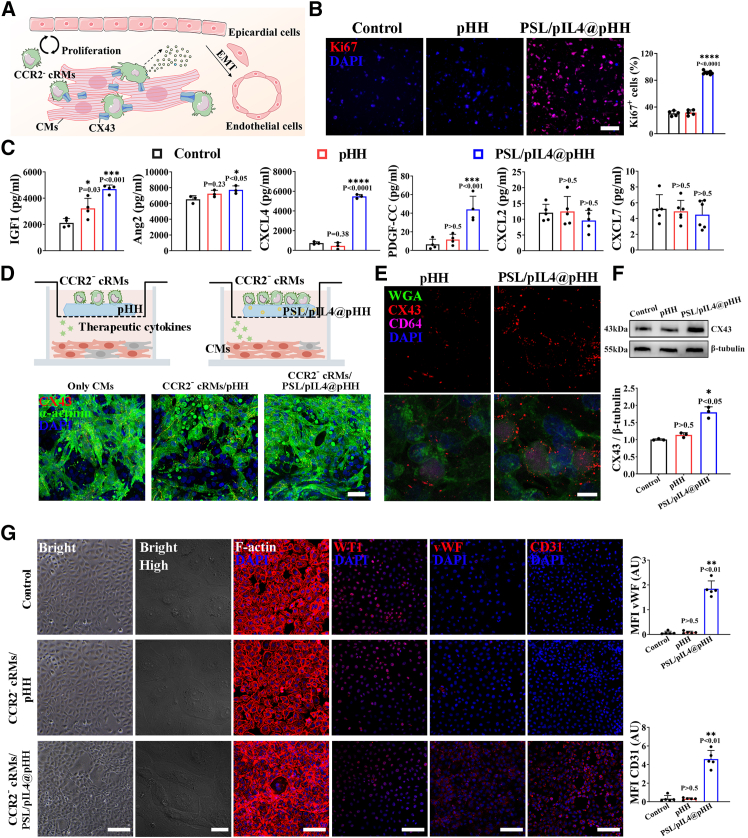
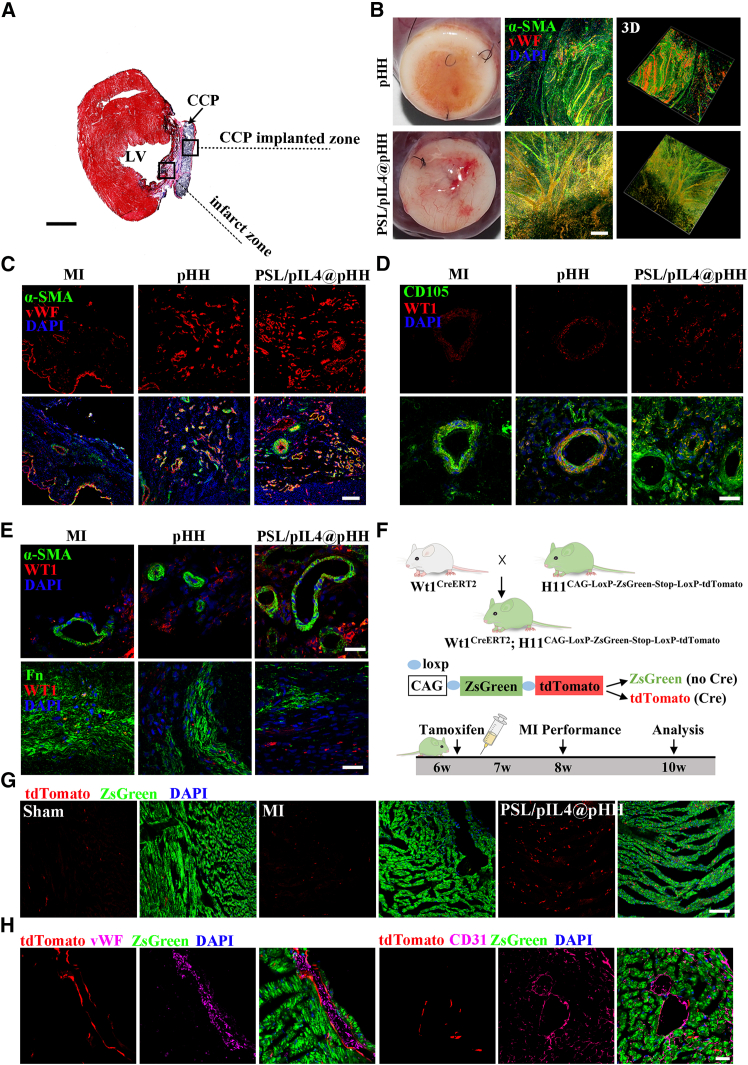
C-C chemokine receptor type 2 (CCR2-) cardiac-resident macrophages (CCR2- cRMs) are known to promote cardiac repair after myocardial infarction (MI). However, the substantial depletion and slow recovery of CCR2- cRMs pose significant barriers in cardiac recovery. Here, we construct a functional conductive cardiac patch (CCP) that can provide exogenously elastic conductive microenvironment and induce endogenously reparative microenvironment mediated by CCR2- cRMs for MI repair. This CCP exhibits suitable mechanical properties, conductivity, and high water retention, reminiscent of natural myocardium, which can actively engage in modulating CCR2- cRM renewal and their cell crosstalk. The functional CCP can promote the expression of Connexin43 between CCR2- cRMs and cardiomyocytes (CMs) and regulate paracrine signaling to activate epicardial cell epithelial-to-mesenchymal transition (EMT) toward endothelial cells using rat and Wt1CreERT2 transgenic lineage tracing mice. Overall, this study provides a promising strategy to construct a synergistic reparative microenvironment for MI repair.
Keywords: cardiac-resident macrophage; cell crosstalk; conductive cardiac patch; epicardial cell; myocardial infarction; revascularization.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures





References
-
- Shin S.H., Hung C.L., Uno H., Hassanein A.H., Verma A., Bourgoun M., Køber L., Ghali J.K., Velazquez E.J., Califf R.M., et al. Mechanical dyssynchrony after myocardial infarction in patients with left ventricular dysfunction, heart failure, or both. Circulation. 2010;121:1096–1103. doi: 10.1161/circulationaha.109.863795. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
