

Inpatient versus outpatient diagnosis of heart failure across the spectrum of ejection fraction: a population cohort study
- PMID: 39880470
- PMCID: PMC12171480
- DOI: 10.1136/heartjnl-2024-324160
Inpatient versus outpatient diagnosis of heart failure across the spectrum of ejection fraction: a population cohort study
Abstract
Background: Early heart failure (HF) diagnosis is crucial to ensure that optimal guideline-directed medical therapy (GDMT) is administered to reduce morbidity and mortality. Limited access to echocardiography could lead to a later diagnosis for patients, for example, during an HF hospitalisation (hHF). This study aimed to compare the incidence and outcomes of inpatient versus outpatient diagnosis of HF.
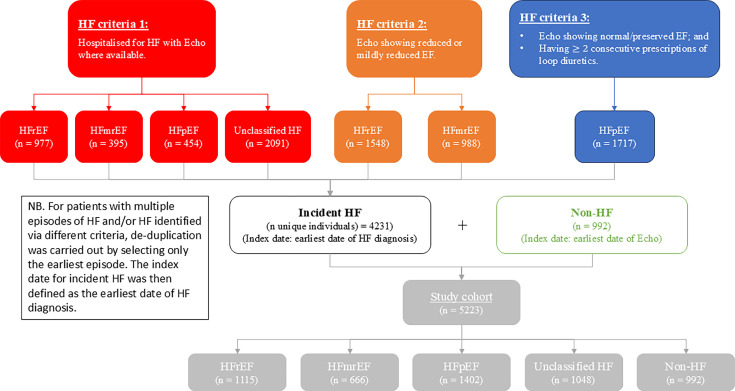
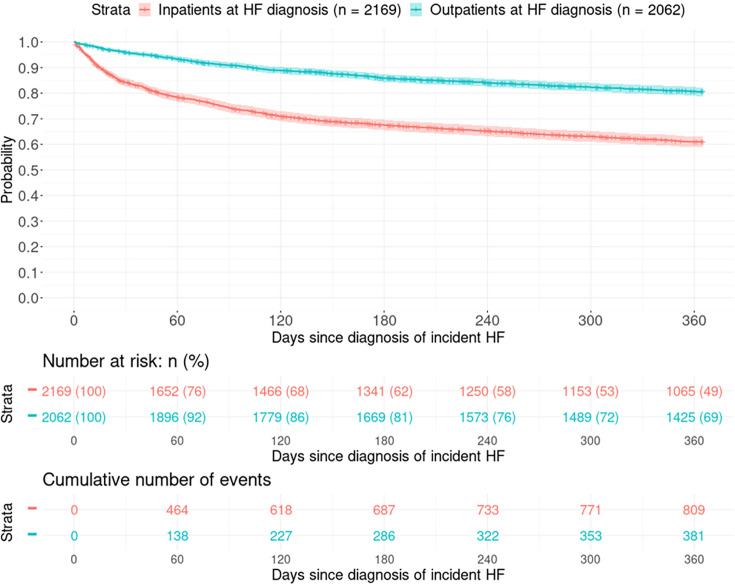
Methods: Electronic health records were linked to echocardiography data between 2015 and 2021 from patients in Tayside, Scotland (population~450 000). Incident HF diagnosis was classified into inpatient or outpatient and stratified by ejection fraction (EF). A non-HF comparator group with normal left ventricular function was also defined. The primary outcome was time to cardiovascular death or hHF within 12 months of diagnosis.
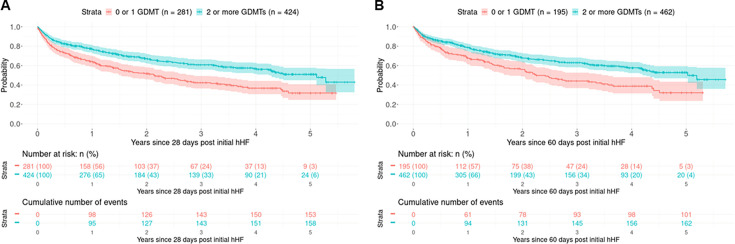
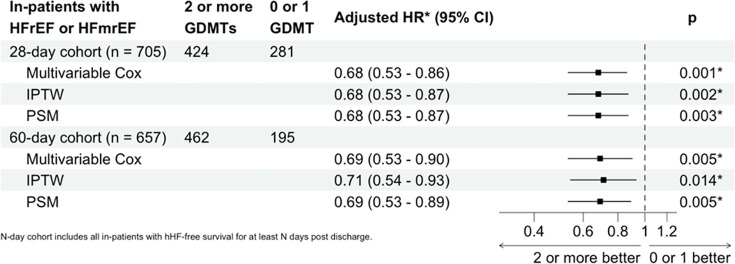
Results: In total, 5223 individuals were identified, 4231 with HF (1115 heart failure with reduced ejection fraction (HFrEF), 666 heart failure with mildly reduced ejection fraction, 1402 heart failure with preserved ejection fraction and 1048 HF with unknown EF) and 992 with non-HF comparators. Of the 4231 HF patients, 2169 (51.3%) were diagnosed as inpatients. The primary outcome was observed in 1193 individuals with HF (28.1%) and 32 (3.2%) non-HF comparators and was significantly more likely to occur in individuals diagnosed as inpatients than outpatients (809 vs 384 events; adjusted HR: 1.62 (1.39-1.89), p<0.001), and this was consistent regardless of EF. For HFrEF patients first diagnosed as inpatients, those discharged on ≥2 GDMT had a reduced incidence of the primary outcome compared with those discharged on <2 GDMT (303 vs 175 events; adjusted HR: 0.72 (0.55-0.94), p=0.016).
Conclusions: Individuals whose first presentation was a HF hospitalisation had a significantly worse outcome than those who were diagnosed in the community. Among hospitalised individuals, higher use of GDMT was associated with improved outcomes. Our results highlight the importance of improving diagnostic pathways to allow for earlier identification and treatment of HF.
Keywords: Electronic Health Records; Heart Failure; Heart failure.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: IRM has received honoraria from AstraZeneca and Novartis. CCL declares receiving consultancy fees and/or research grants from Amgen, AstraZeneca, MSD, Novartis and Servier. All other authors have no conflict of interest to declare.
Figures
Similar articles
-
Outcomes of KDIGO-Defined CKD in U.S. Veterans With HFpEF, HFmrEF, and HFrEF.JACC Heart Fail. 2025 Mar;13(3):467-479. doi: 10.1016/j.jchf.2024.11.007. Epub 2025 Feb 5. JACC Heart Fail. 2025. PMID: 39918536
-
Contemporary Guideline-Directed Medical Therapy and Outpatient Worsening Heart Failure Events in Hospitalized Patients With Heart Failure - Preliminary Observational Study on Utilizing Predischarge Period for Optimizing Medications in Hospitalized Patients With Heart Failure (PRE-UPFRONT-HF).Circ J. 2025 Jun 25;89(7):912-920. doi: 10.1253/circj.CJ-24-1020. Epub 2025 May 11. Circ J. 2025. PMID: 40350293
-
Guideline-Directed Medical Therapy and Outcomes Among Patients With Heart Failure With Improved Ejection Fraction.J Am Coll Cardiol. 2025 Aug 5;86(5):338-350. doi: 10.1016/j.jacc.2025.05.040. J Am Coll Cardiol. 2025. PMID: 40738561
-
Systematic review and meta-analysis of stroke and thromboembolism risk in atrial fibrillation with preserved vs. reduced ejection fraction heart failure.BMC Cardiovasc Disord. 2024 Sep 18;24(1):495. doi: 10.1186/s12872-024-04133-1. BMC Cardiovasc Disord. 2024. PMID: 39289613 Free PMC article.
-
Pharmacological Treatments in Heart Failure With Mildly Reduced and Preserved Ejection Fraction: Systematic Review and Network Meta-Analysis.JACC Heart Fail. 2024 Apr;12(4):616-627. doi: 10.1016/j.jchf.2023.07.014. Epub 2023 Aug 30. JACC Heart Fail. 2024. PMID: 37656079
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous