

Intricacies of human-AI interaction in dynamic decision-making for precision oncology
- PMID: 39881134
- PMCID: PMC11779952
- DOI: 10.1038/s41467-024-55259-x
Intricacies of human-AI interaction in dynamic decision-making for precision oncology
Abstract
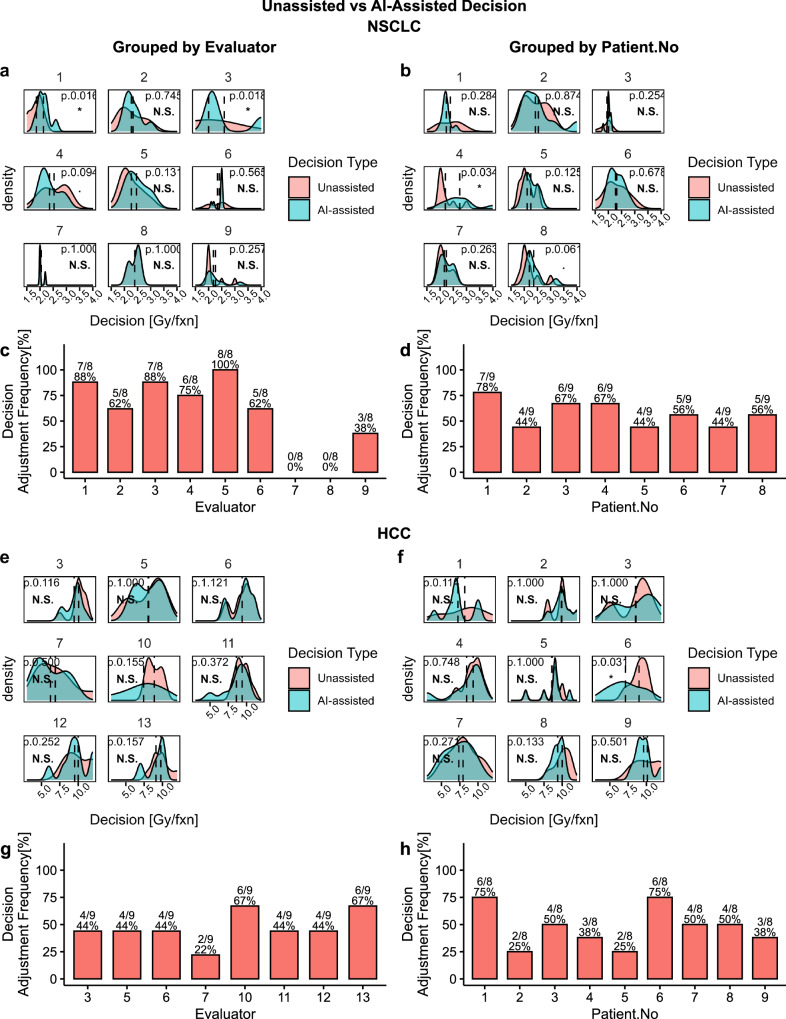
AI decision support systems can assist clinicians in planning adaptive treatment strategies that can dynamically react to individuals' cancer progression for effective personalized care. However, AI's imperfections can lead to suboptimal therapeutics if clinicians over or under rely on AI. To investigate such collaborative decision-making process, we conducted a Human-AI interaction study on response-adaptive radiotherapy for non-small cell lung cancer and hepatocellular carcinoma. We investigated two levels of collaborative behavior: model-agnostic and model-specific; and found that Human-AI interaction is multifactorial and depends on the complex interrelationship between prior knowledge and preferences, patient's state, disease site, treatment modality, model transparency, and AI's learned behavior and biases. In summary, some clinicians may disregard AI recommendations due to skepticism; others will critically analyze AI recommendations on a case-by-case basis; clinicians will adjust their decisions if they find AI recommendations beneficial to patients; and clinician will disregard AI recommendations if deemed harmful or suboptimal and seek alternatives.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: DN, KCC, IDD, JBJ, JJ, YL, RKTH, AKB, MPD, JMF, CLL, SRM, MNM, RFP, SNR, and AR have no conflicting interests. BDG reports fees unrelated to this work from Sure Med Compliance and Elly Health. MMM reports research funding from Varian, a licensing agreement with Fuse Oncology, and serves in the AAPM Board of Directors and is the Co-Director of MROQC, funded by BCBSM. TJD is a member of the National Comprehensive Cancer Network (NCCN) NSCLC panel. JFTR reports stock ownership and leadership in Cvergenx, Inc. He reports IP and royalty rights in RSI, GARD, RxRSI. HHMY reports funding or fees unrelated to this work from the National Institute of Health, UpToDate, Novocure and Bristol-Myers Squib. IEN is on the scientific advisory of Endectra, LLC., co-founder of iRAI LLC, deputy editor for the journal of Medical Physics, co-chief editor of British Journal of Radiology (BJR)-AI and receives funding from the National Institute of Health (NIH), foundations, and Department of Defense (DoD). A PCT patent application for ARCliDS has been filed. Patent Title: Adaptive radiotherapy clinical decision support tool and related methods, Patent Applicant: H Lee Moffitt Cancer Center IP office in conjunction with University of Michigan IP office. Inventors: DN, IEN, RKTH, Wenbo Sun, JJ, IDD, KCC, MMM, and JBJ. Application Number: US2023/075004. Status of Application: Pending. Specific aspect of manuscript covered in patent application: The patent covers the underlying model-based decision-making framework of ARCliDS.
Figures







Update of
-
Intricacies of Human-AI Interaction in Dynamic Decision-Making for Precision Oncology: A Case Study in Response-Adaptive Radiotherapy.medRxiv [Preprint]. 2024 Apr 30:2024.04.27.24306434. doi: 10.1101/2024.04.27.24306434. medRxiv. 2024. Update in: Nat Commun. 2025 Jan 29;16(1):1138. doi: 10.1038/s41467-024-55259-x. PMID: 38746238 Free PMC article. Updated. Preprint.
References
-
- Scott, E. C. et al. Trends in the approval of cancer therapies by the FDA in the twenty-first century. Nat. Rev. Drug Discov.22, 625–640 (2023). - PubMed
-
- Adaptive Treatment Strategies in Practice. (Society for Industrial and Applied Mathematics, Philadelphia, PA). 10.1137/1.9781611974188 (2015).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
