

Anti-inflammatory coupled anti-angiogenic airway stent effectively suppresses tracheal in-stents restenosis
- PMID: 39881307
- PMCID: PMC11776288
- DOI: 10.1186/s12951-024-03087-y
Anti-inflammatory coupled anti-angiogenic airway stent effectively suppresses tracheal in-stents restenosis
Abstract
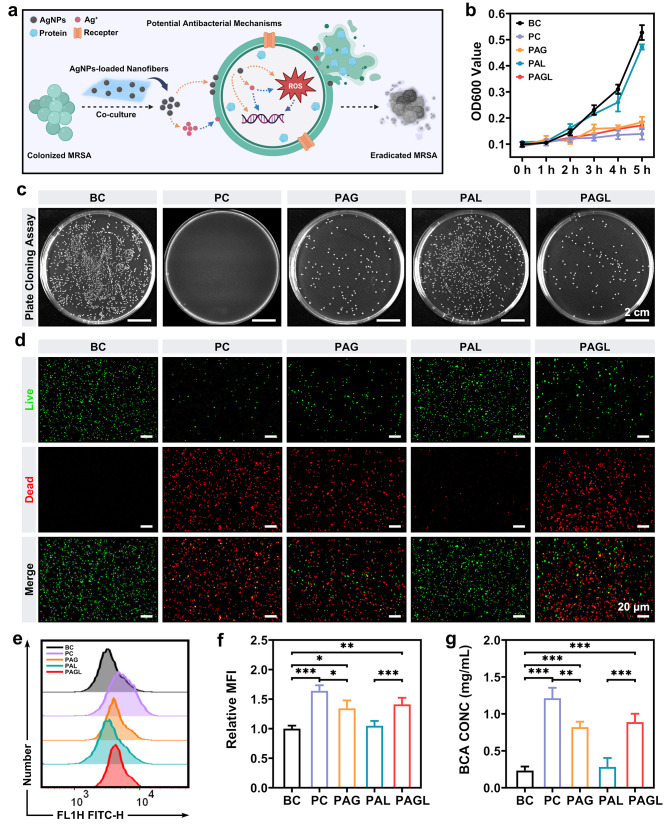
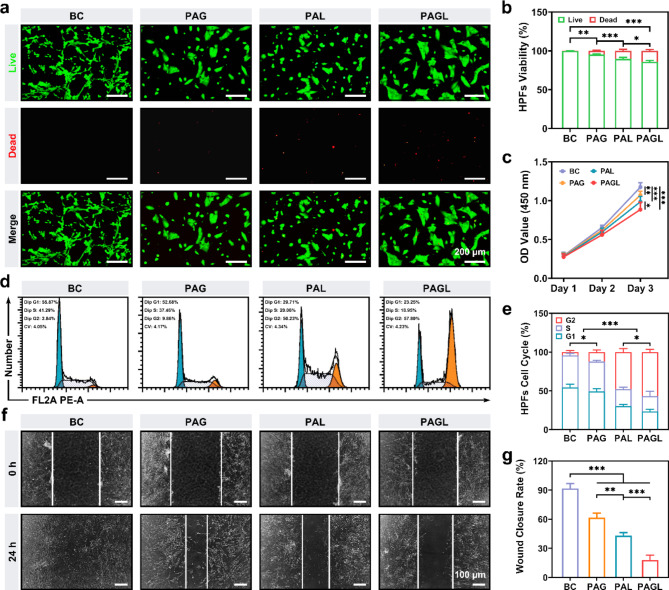
Excessive vascularization during tracheal in-stent restenosis (TISR) is a significant but frequently overlooked issue. We developed an anti-inflammatory coupled anti-angiogenic airway stent (PAGL) incorporating anlotinib hydrochloride and silver nanoparticles using advanced electrospinning technology. PAGL exhibited hydrophobic surface properties, exceptional mechanical strength, and appropriate drug-release kinetics. Moreover, it demonstrated a remarkable eradication effect against methicillin-resistant Staphylococcus aureus. It also displayed anti-proliferative and anti-angiogenic properties on human umbilical vein endothelial cells and lung fibroblasts. PAGL was implanted into the tracheae of New Zealand rabbits to evaluate its efficacy in inhibiting bacterial infection, suppressing the inflammatory response, reducing angiogenesis, and attenuating excessive fibroblast activation. RNA sequencing analysis revealed a significant downregulation of genes associated with fibrosis, intimal hyperplasia, and cell migration following PAGL treatment. This study provides insight into the development of airway stents that target angiogenesis and inflammation to address problems associated with TISR effectively and have the potential for clinical translation.
Keywords: Airway stent; Anlotinib; Silver nanoparticles; Tracheal in-stents restenosis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All animal experiments were granted approval by the animal care committee of the First Affiliated Hospital of Zhengzhou University (2023042602). Consent for publication: Written informed consent for publication was obtained from all participants. Competing interests: The authors declare no competing interests.
Figures






References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
