

Effectiveness and Safety in Patients with Non-Valvular Atrial Fibrillation Who Switched from Warfarin to Direct Oral Anticoagulants in Medicare Population
- PMID: 39883308
- PMCID: PMC11868198
- DOI: 10.1007/s12325-024-03099-y
Effectiveness and Safety in Patients with Non-Valvular Atrial Fibrillation Who Switched from Warfarin to Direct Oral Anticoagulants in Medicare Population
Abstract
Introduction: Atrial fibrillation (AF), a common heart rhythm abnormality, is linked to a higher risk of stroke. Traditionally, warfarin has been the primary anticoagulation treatment for reducing the stroke risk. The new standard of treatment by direct oral anticoagulants (DOACs) offers greater benefits including improved efficacy and fewer adverse effects with reduced monitoring. This study aims to evaluate the risk of stroke/systemic embolism (SE) and major bleeding (MB) among patients with AF who switched from warfarin to DOACs.
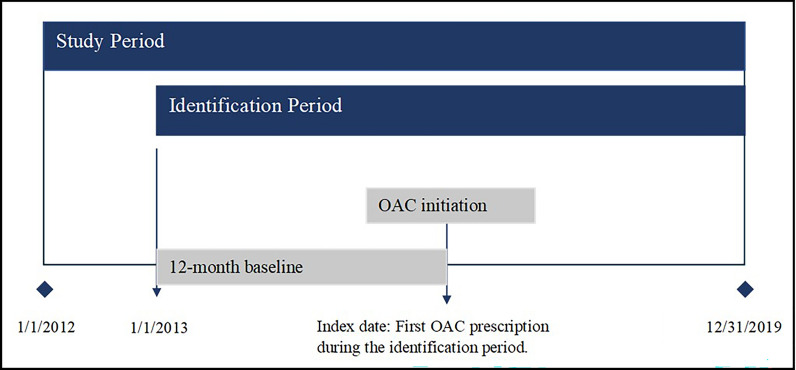
Methods: This study utilized Medicare data to conduct a retrospective analysis of patients with non-valvular atrial fibrillation (NVAF) who switched from warfarin to DOACs between January 1, 2012, and December 31, 2019. Patients with NVAF aged 65 and older who switched from warfarin and had continuous health plan enrollment were included. Descriptive statistics, propensity score matching (PSM), and Cox proportional hazard (PH) models were utilized to compare the outcomes and assess risks of SE and MB across the DOAC cohorts.
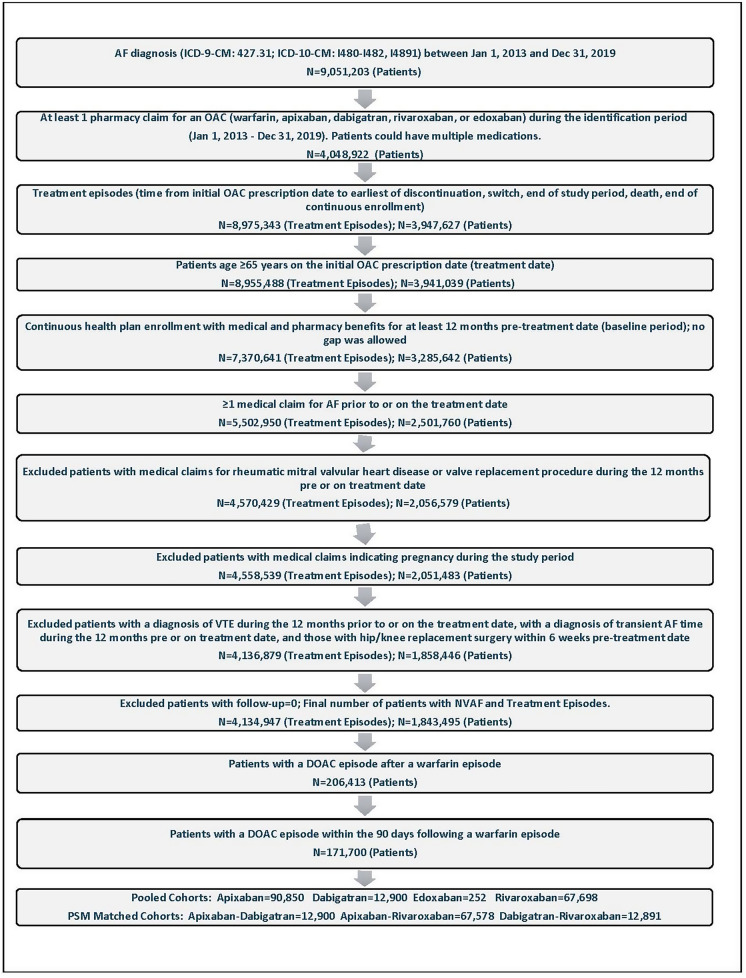
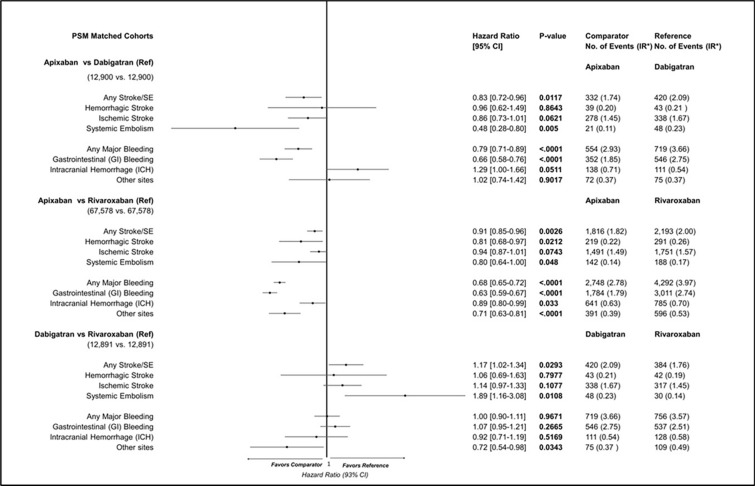
Results: Among 1,843,495 patients with NVAF on warfarin, 171,700 switched to DOACs within 90 days of discontinuation (apixaban: 90,850; rivaroxaban: 67,698; dabigatran: 12,900). The mean follow-up period across DOAC cohorts ranged from 552 to 628 days. After PSM, apixaban showed significantly lower rates of stroke/SE compared to dabigatran (2.99% vs. 3.98%, p < 0.0001) and rivaroxaban (3.08% vs. 3.80%, p < 0.0001). MB rates were also lower with apixaban versus dabigatran (4.29% vs. 5.57%, p < 0.0001) and rivaroxaban (4.07% vs. 6.35%, p < 0.0001). Cox PH models confirmed these findings, with apixaban demonstrating lower risks of stroke/SE [hazard ratio (HR) 0.83, 95% confidence interval (CI) 0.72-0.96 vs. dabigatran; HR 0.91, 95% CI 0.85-0.96 vs. rivaroxaban] and MB (HR 0.79, 95% CI 0.71-0.89 vs. dabigatran; HR 0.68, 95% CI 0.65-0.72 vs. rivaroxaban).
Conclusion: The risk of stroke/SE and MB varies significantly among patients with NVAF switching from warfarin to different DOACs, with apixaban presenting the lowest risk compared to dabigatran and rivaroxaban.
Keywords: Apixaban; Atrial fibrillation; Dabigatran; Direct oral anticoagulants; Rivaroxaban; Stroke; Switch; Systemic embolism; Warfarin.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: Anandkumar Dubey, Amiee Kang, Jenny Jiang, and Dong Cheng are employees of BMS and may hold stock options. Nipun Atreja and Melissa Hagan were employees of BMS when the study was conducted. Nipun Atreja is currently affiliated with Immunovant. Melissa Hagan is currently affiliated with BeiGene. Abimbola Michael-Asalu is an employee of STATinMED. Steven Deitelzweig received research and consulting support from Pfizer and BMS. Ethical Approval: Since this study did not involve the collection, use, or transmittal of individually identifiable data, Institutional Review Board (IRB) approval was not required. This study only analyzed de-identified data which are a priori exempt from the Federal Policy for the Protection of Human Subjects (1991) and do not meet the identification criteria necessary to be privileged under the Health Insurance Portability and Accountability Act (HIPAA). Both the data and the security of the offices where the data were kept met HIPAA requirements. All authors had permission to access and use the database utilized in this study.
Figures
References
-
- Healthline. What is nonvalvular atrial fibrillation? 2023 [updated 5/19/2023. Available from: https://www.healthline.com/health/atrial-fibrillation/nonvalvular.
-
- Gilligan AM, Gandhi P, Song X, Wang C, Henriques C, Sander S, et al. All-cause, stroke-, and bleed-specific healthcare costs: comparison among patients with non-valvular atrial fibrillation (NVAF) newly treated with dabigatran or warfarin. Am J Cardiovasc Drugs. 2017;17(6):481–92. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
