

Risk Factors for Gastrointestinal Bleeding in Patients With Acute Myocardial Infarction: Multicenter Retrospective Cohort Study
- PMID: 39883922
- PMCID: PMC11826945
- DOI: 10.2196/67346
Risk Factors for Gastrointestinal Bleeding in Patients With Acute Myocardial Infarction: Multicenter Retrospective Cohort Study
Abstract
Background: Gastrointestinal bleeding (GIB) is a severe and potentially life-threatening complication in patients with acute myocardial infarction (AMI), significantly affecting prognosis during hospitalization. Early identification of high-risk patients is essential to reduce complications, improve outcomes, and guide clinical decision-making.
Objective: This study aimed to develop and validate a machine learning (ML)-based model for predicting in-hospital GIB in patients with AMI, identify key risk factors, and evaluate the clinical applicability of the model for risk stratification and decision support.
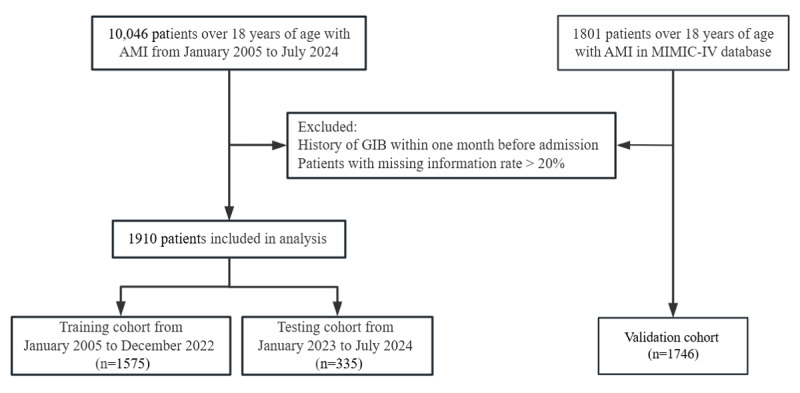
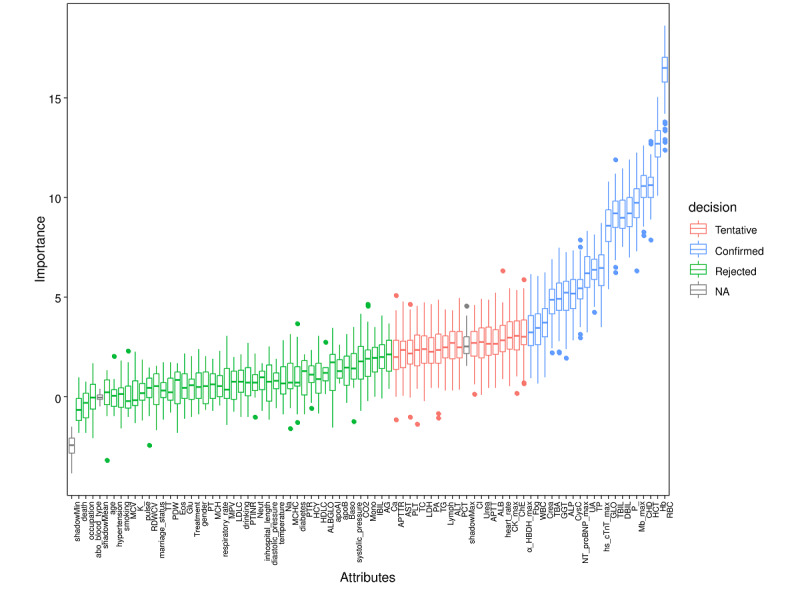
Methods: A multicenter retrospective cohort study was conducted, including 1910 patients with AMI from the Affiliated Hospital of Guangdong Medical University (2005-2024). Patients were divided into training (n=1575) and testing (n=335) cohorts based on admission dates. For external validation, 1746 patients with AMI were included in the publicly available MIMIC-IV (Medical Information Mart for Intensive Care IV) database. Propensity score matching was adjusted for demographics, and the Boruta algorithm identified key predictors. A total of 7 ML algorithms-logistic regression, k-nearest neighbors, support vector machine, decision tree, random forest (RF), extreme gradient boosting, and neural networks-were trained using 10-fold cross-validation. The models were evaluated for the area under the receiver operating characteristic curve, accuracy, sensitivity, specificity, recall, F1-score, and decision curve analysis. Shapley additive explanations analysis ranked variable importance. Kaplan-Meier survival analysis evaluated the impact of GIB on short-term survival. Multivariate logistic regression assessed the relationship between coronary heart disease (CHD) and in-hospital GIB after adjusting for clinical variables.
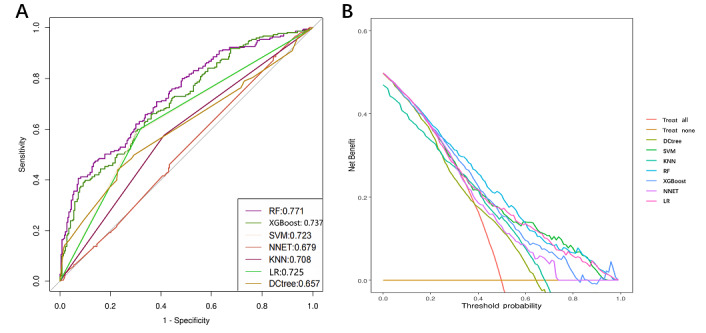
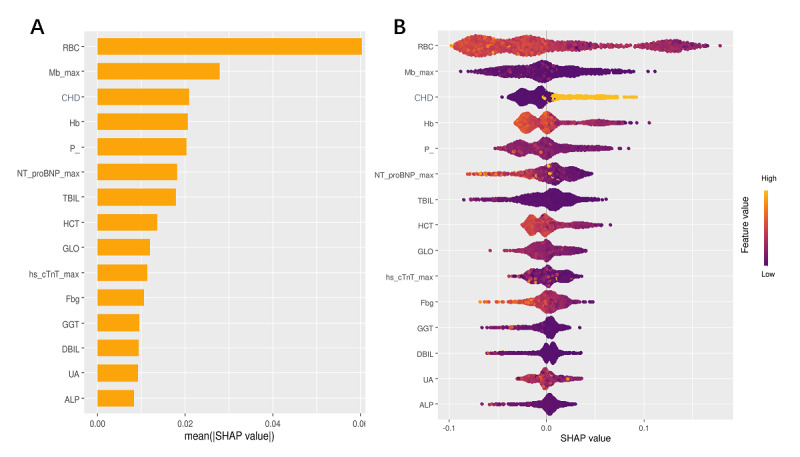
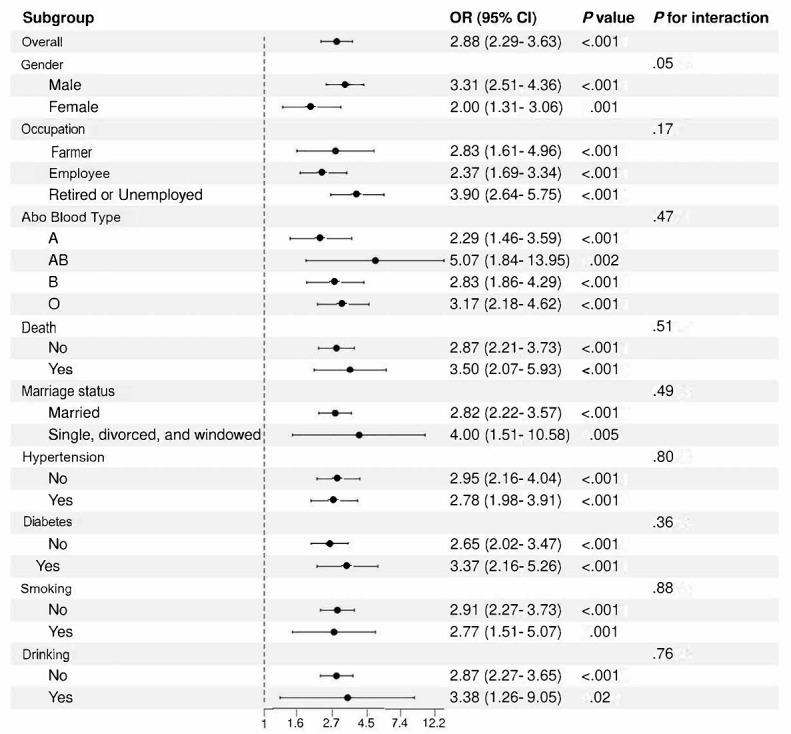
Results: The RF model outperformed other ML models, achieving an area under the receiver operating characteristic curve of 0.77 in the training cohort, 0.77 in the testing cohort, and 0.75 in the validation cohort. Key predictors included red blood cell count, hemoglobin, maximal myoglobin, hematocrit, CHD, and other variables, all of which were strongly associated with GIB risk. Decision curve analysis demonstrated the clinical use of the RF model for early risk stratification. Kaplan-Meier survival analysis showed no significant differences in 7- and 15-day survival rates between patients with AMI with and without GIB (P=.83 for 7-day survival and P=.87 for 15-day survival). Multivariate logistic regression showed that CHD was an independent risk factor for in-hospital GIB (odds ratio 2.79, 95% CI 2.09-3.74). Stratified analyses by sex, age, occupation, marital status, and other subgroups consistently showed that the association between CHD and GIB remained robust across all subgroups.
Conclusions: The ML-based RF model provides a robust and clinically applicable tool for predicting in-hospital GIB in patients with AMI. By leveraging routinely available clinical and laboratory data, the model supports early risk stratification and personalized preventive strategies.
Keywords: acute myocardial infarction; gastrointestinal bleeding; in-hospital; machine learning; prediction model.
©Yanqi Kou, Shicai Ye, Yuan Tian, Ke Yang, Ling Qin, Zhe Huang, Botao Luo, Yanping Ha, Liping Zhan, Ruyin Ye, Yujie Huang, Qing Zhang, Kun He, Mouji Liang, Jieming Zheng, Haoyuan Huang, Chunyi Wu, Lei Ge, Yuping Yang. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 30.01.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Application of an interpretable machine learning method to predict the risk of death during hospitalization in patients with acute myocardial infarction combined with diabetes mellitus.Acta Cardiol. 2025 Jun;80(4):358-375. doi: 10.1080/00015385.2025.2481662. Epub 2025 Apr 8. Acta Cardiol. 2025. PMID: 40195951
-
Development and Validation of Machine Learning Models for Predicting 7-Day Mortality in Critically Ill Patients with Traumatic Spinal Cord Injury: A Multicenter Retrospective Study.Neurocrit Care. 2025 Jun 25. doi: 10.1007/s12028-025-02308-y. Online ahead of print. Neurocrit Care. 2025. PMID: 40563047
-
Machine Learning for the Prediction of Acute Kidney Injury in Critically Ill Patients With Coronary Heart Disease: Algorithm Development and Validation.JMIR Med Inform. 2025 May 28;13:e72349. doi: 10.2196/72349. JMIR Med Inform. 2025. PMID: 40383933 Free PMC article.
-
Predicting acute kidney injury risk in acute myocardial infarction patients: An artificial intelligence model using medical information mart for intensive care databases.Front Cardiovasc Med. 2022 Sep 7;9:964894. doi: 10.3389/fcvm.2022.964894. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36158815 Free PMC article.
-
The CMLA score: A novel tool for early prediction of renal replacement therapy in patients with cardiogenic shock.Curr Probl Cardiol. 2024 Dec;49(12):102870. doi: 10.1016/j.cpcardiol.2024.102870. Epub 2024 Sep 27. Curr Probl Cardiol. 2024. PMID: 39343053 Review.
Cited by
-
The future of critical care: AI-powered mortality prediction for acute variceal gastrointestinal bleeding and acute non-variceal gastrointestinal bleeding patients.Front Med (Lausanne). 2025 May 16;12:1580094. doi: 10.3389/fmed.2025.1580094. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40454154 Free PMC article.
References
-
- Martin SS, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, Baker-Smith CM, Barone Gibbs B, Beaton AZ, Boehme AK, Commodore-Mensah Y, Currie ME, Elkind MSV, Evenson KR, Generoso G, Heard DG, Hiremath S, Johansen MC, Kalani R, Kazi DS, Ko D, Liu J, Magnani JW, Michos ED, Mussolino ME, Navaneethan SD, Parikh NI, Perman SM, Poudel R, Rezk-Hanna M, Roth GA, Shah NS, St-Onge M, Thacker EL, Tsao CW, Urbut SM, Van Spall HGC, Voeks JH, Wang N, Wong ND, Wong SS, Yaffe K, Palaniappan LP. 2024 heart disease and stroke statistics: a report of US and Global Data From the American Heart Association. Circulation. 2024;149(8):e347–e913. doi: 10.1161/CIR.0000000000001209. https://www.ahajournals.org/doi/abs/10.1161/CIR.0000000000001209?url_ver... - DOI - DOI - PubMed
-
- Oakland K, Kahan BC, Guizzetti L, Martel M, Bryant RV, Brahmania M, Singh S, Nguyen NQ, Sey MSL, Barkun A, Jairath V. Development, validation, and comparative assessment of an international scoring system to determine risk of upper gastrointestinal bleeding. Clin Gastroenterol Hepatol. 2019;17(6):1121–1129.e2. doi: 10.1016/j.cgh.2018.09.039.S1542-3565(18)31069-3 - DOI - PubMed
-
- Bilal M, Samuel R, Khalil MK, Singh S, Parupudi S, Abougergi MS. Nonvariceal upper GI hemorrhage after percutaneous coronary intervention for acute myocardial infarction: a national analysis over 11 months. Gastrointest Endosc. 2020;92(1):65–74.e2. doi: 10.1016/j.gie.2020.01.039.S0016-5107(20)30097-3 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
