

Discriminatory power of trabeculectomy bleb internal reflectivity and morphology in surgical success using anterior segment optical coherence tomography
- PMID: 39885439
- PMCID: PMC11780981
- DOI: 10.1186/s12886-024-03770-6
Discriminatory power of trabeculectomy bleb internal reflectivity and morphology in surgical success using anterior segment optical coherence tomography
Abstract
Background: The post-operative evaluation of trabeculectomy blebs has traditionally relied on subjective clinical grading systems performed at the slit-lamp. This study explores the use of swept source anterior-segment optical coherence tomography (AS-OCT) to objectively measure bleb internal reflectivity and morphology, and to distinguish blebs with surgical success vs. failure.
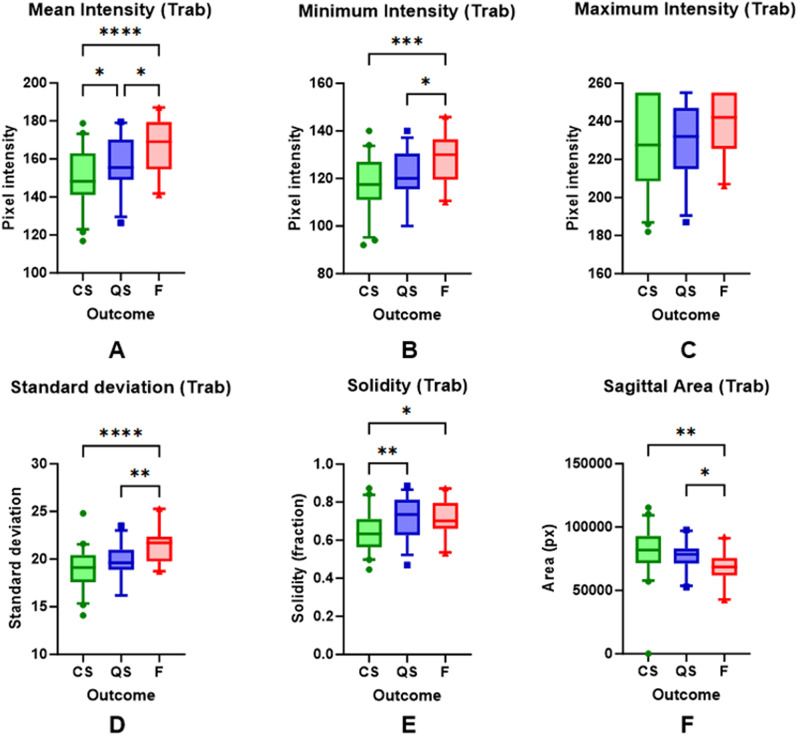
Methods: Cross-sectional study of patients with glaucoma who had undergone trabeculectomy at least one year prior. Swept source AS-OCT was used to capture filtering blebs in the sagittal plane. Standardised regions of interests on the sagittal plane were segmented, and pixel intensity values and bleb height were measured. Receiver operating characteristic curves were used to examine the discriminatory ability of pixel intensity values and bleb morphology to classify blebs with surgical success or failure.
Results: 100 eyes of 65 patients were included, with a median post-operative follow up of 7.0 years (IQR 3.2-16 years). The proportion of complete success, qualified success and failure was 45%, 33%, and 22% respectively. The maximum bleb height was significantly greater in the blebs with complete success (1.74 vs. 1.25 vs. 1.23 mm in CS vs. QS vs. F, one-way ANOVA, p < 0.0001). Mean pixel intensity was significantly lower in blebs with complete success (150.8 vs. 157.4 vs. 167.4 in CS vs. QS vs. F, p = 0.0001). Bleb intensity standard deviation (AUC 0.81), maximal bleb height (AUC 0.76), mean pixel intensity (AUC 0.75) and minimum pixel intensity (AUC 0.75) offered the best discrimination between surgical success and failure.
Conclusions: Swept-source AS-OCT can be used to quantify bleb internal reflectivity and morphology, which can be used to distinguish between well vs. poorly functioning blebs. These parameters may assist surgeons in the objective evaluation of post-operative bleb outcomes.
Keywords: Glaucoma surgery; Mitomycin-C; Scleral flap; Sclerostomy; Surgical success; Surgical technique; Trabeculectomy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Royal Liverpool University Hospital Trust clinical governance department (reference number: 11783). Due to the retrospective nature of this study using deidentified data, waiver of consent was granted by the Royal Liverpool University Hospital Trust clinical governance department; informed consent was not required from participants. Consent for publication: Not applicable. Meeting presentation: Presented at the Association for Research in Vision and Ophthalmology Annual meeting 2023, New Orleans, Louisiana. Competing interests: The authors declare no competing interests.
Figures




References
-
- Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–90. - PubMed
-
- Khaw PT, Chiang M, Shah P, Sii F, Lockwood A, Khalili A. Enhanced trabeculectomy: the Moorfields Safer surgery system. Dev Ophthalmol. 2017;59:15–35. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
