

Multiomics unravels the complexity of male obesity: a prospective observational study
- PMID: 39885510
- PMCID: PMC11783726
- DOI: 10.1186/s12967-024-06040-7
Multiomics unravels the complexity of male obesity: a prospective observational study
Abstract
Background: Obesity is associated with varying degrees of metabolic dysfunction. In this study, we aimed to discover markers of the severity of metabolic impairment in men with obesity via a multiomics approach.
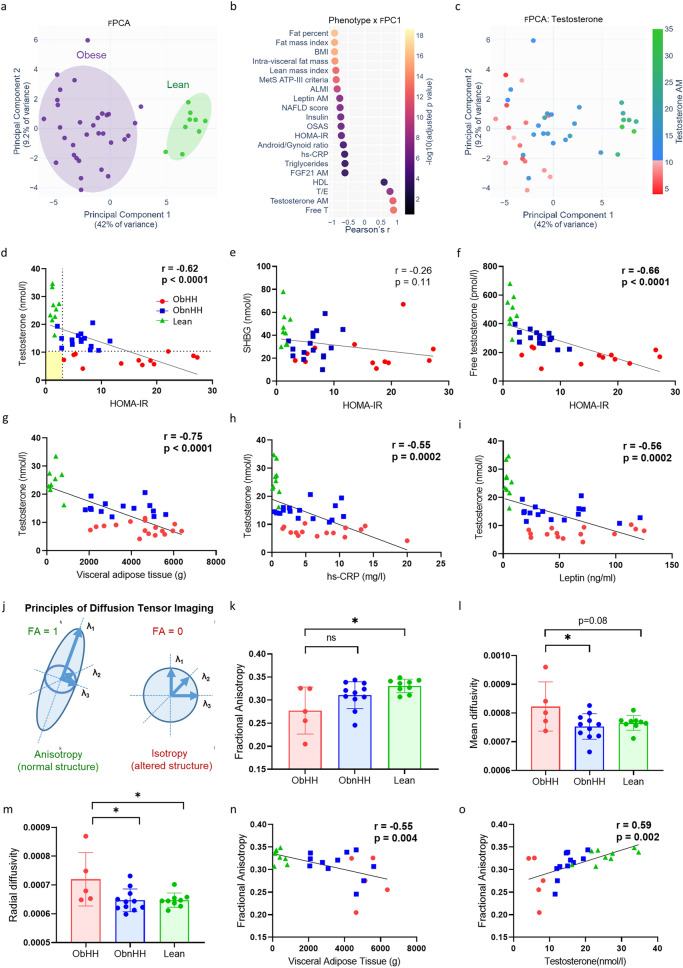
Methods: Thirty-two morbidly men with obesity who were candidates for Roux-en-Y gastric bypass (RYGB) surgery were prospectively followed. Nine healthy adults served as controls. Deep phenotyping, including targeted metabolomics, transcriptomics, and brain magnetic resonance imaging (MRI), was performed.
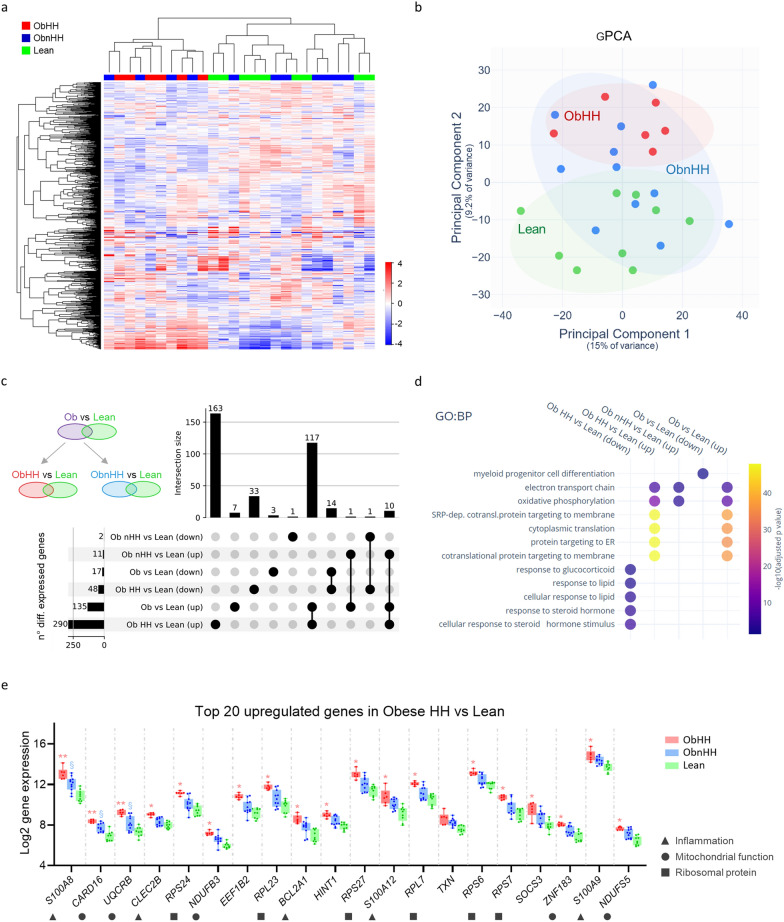
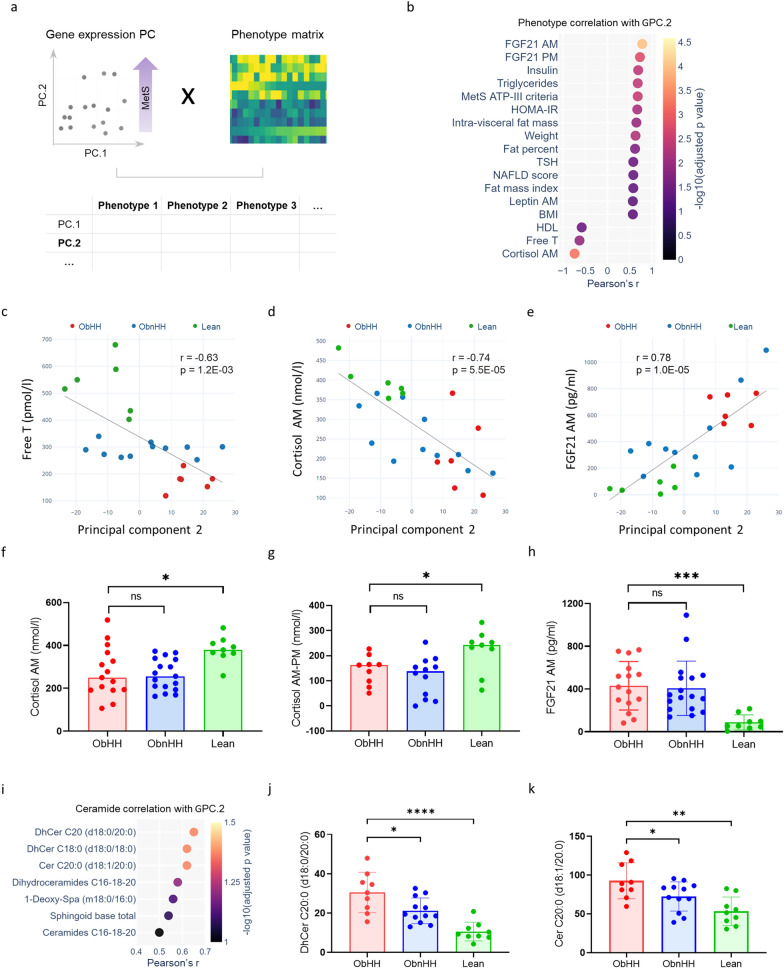
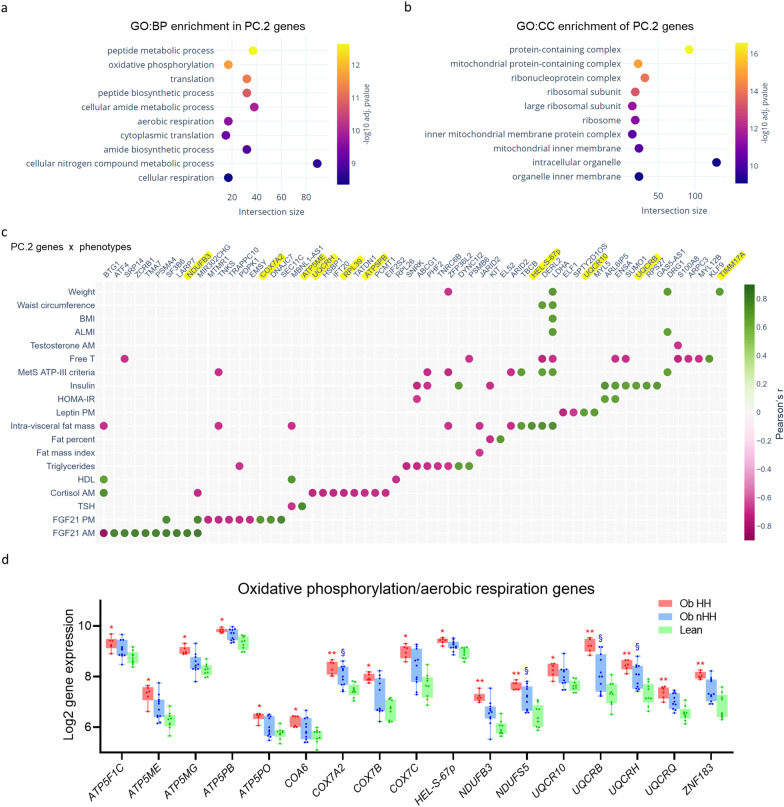
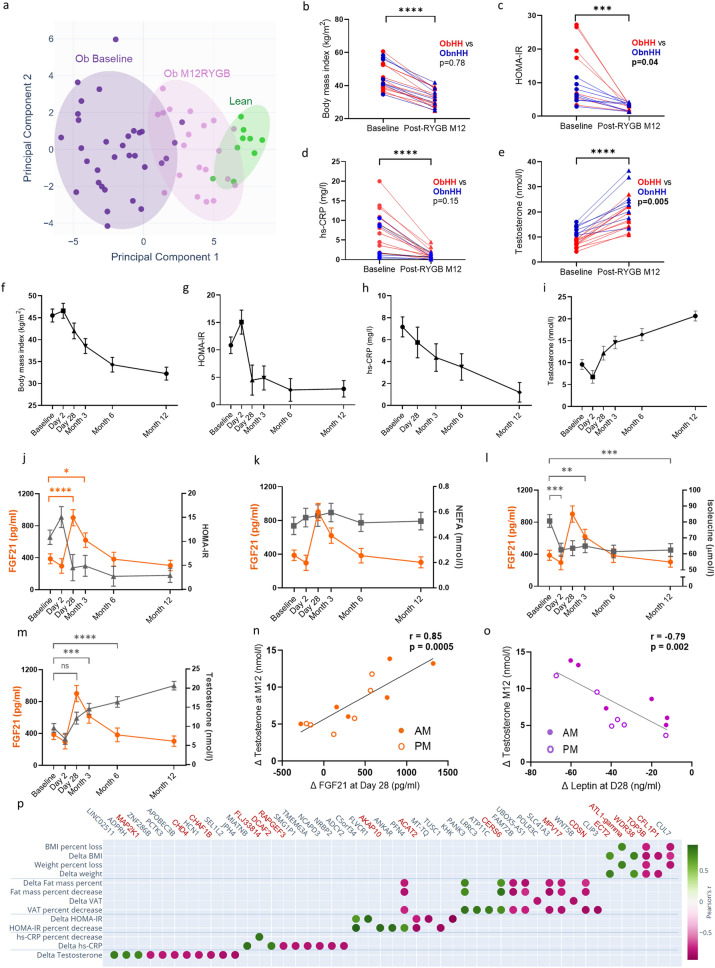
Results: Testosterone emerged as a key contributor to phenotypic variability via principal component analysis and was therefore used to further categorize obese patients as having or not having hypogonadotropic hypogonadism (HH). Despite having comparable body mass indices, obese individuals with HH presented with worse metabolic defects than obese individuals without HH, including higher insulin resistance, as well as MRI signs of hypothalamic inflammation and a specific blood transcriptomics signature. The upregulated genes were involved mainly in inflammation, mitochondrial function, and protein translation. Integration of gene expression and clinical data revealed high FGF21 and low cortisol levels as the top markers correlated with the transcriptomic signature of metabolic risk. Following RYGB-induced substantial weight loss, testosterone levels markedly increased in both obese individuals with and without HH, challenging the current definition of hypogonadism. A longitudinal study in a subset of men with obesity following bariatric surgery revealed a unique FGF21 trajectory with a sharp peak at one month post-RYGB that correlated with metabolic and reproductive improvements.
Conclusions: Combining clinical, biochemical, and molecular markers allows adequate stratification of metabolic risk in men with obesity and provides novel tools for personalized care.
Keywords: Bariatric surgery; Hypogonadism; Male obesity; Metabolic risk stratification; Transcriptomics.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The research protocol was approved by the Institutional Ethics Committee for Research of the Canton of Vaud, Switzerland (CER-VD), and written informed consent was obtained from all participants. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
References
-
- Vermeulen A, Kaufman JM, Deslypere JP, Thomas G. Attenuated luteinizing hormone (LH) pulse amplitude but normal LH pulse frequency, and its relation to plasma androgens in hypogonadism of obese men. J Clin Endocrinol Metab. 1993;76(5):1140–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
