

doi: 10.1111/bju.16670.
Epub 2025 Jan 30.
Extraperitoneal single-site robot-assisted radical prostatectomy with extended pelvic lymph node dissection: technique and experience
Affiliations
- PMID: 39887625
- PMCID: PMC11913595
- DOI: 10.1111/bju.16670
Item in Clipboard
Extraperitoneal single-site robot-assisted radical prostatectomy with extended pelvic lymph node dissection: technique and experience
BJU Int.
2025 Apr.
No abstract available
Keywords: Lymphocele; extended pelvic lymph node dissection; locally advanced prostate cancer; robot‐assisted radical prostatectomy; single site.
Figures

Preoperative preparation of ESSRARP with ePLND. (A) The patient was positioned in a modified Trendelenburg position. (B) The incision was made above the pubic symphysis. (C) The transverse incision was ~5 cm, with a wound protector. (D) The extraperitoneal working space was created with a dilator. Port installation and trocar placement before (E) and after (F) docking.
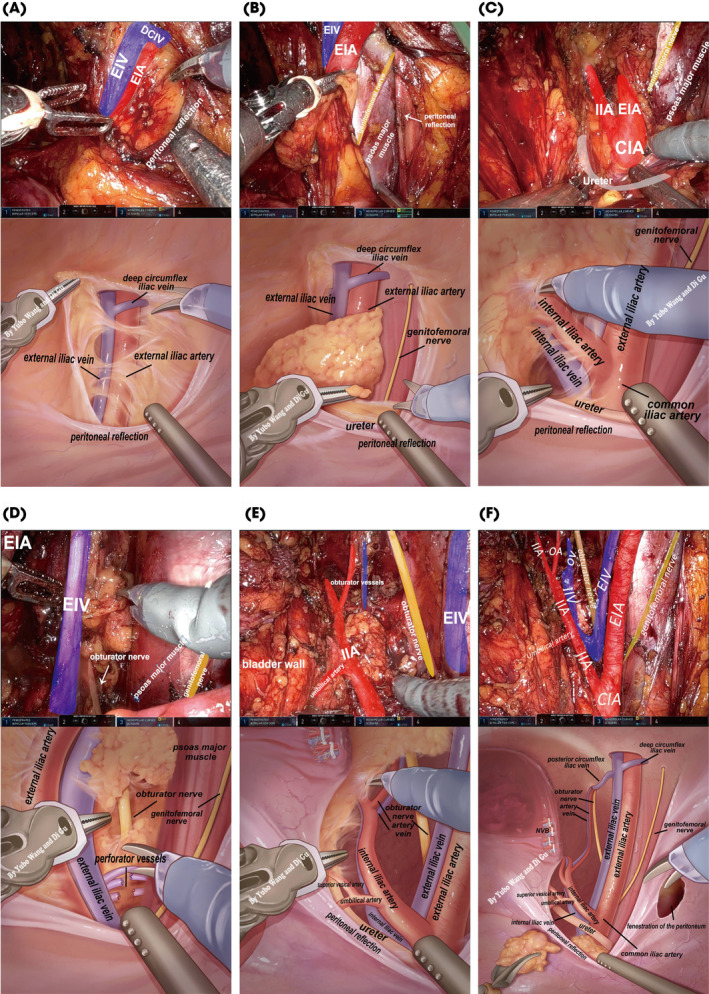
Actual and virtual schematic diagrams of intraoperative steps (ePLND) and important anatomical structure: (A) Determined the deep circumflex iliac vein. (B) Exposed the genitofemoral nerve and psoas major muscle as the lateral limit. (C) Located the common iliac artery bifurcation as the cranial limit. (D) Dissected the external iliac lymph nodes dissection on the lateral side to pretreat perforator vessels and entered the triangle of Marcille to dissect and expose the cranial side of the obturator nerve. (E) The LNs along the internal iliac vessels and the obturator lymphatic tissue were dissected. (F) The surrounding anatomy was skeletonised and performed fenestration of the peritoneum. CIA, common iliac artery; DCIV, deep circumflex iliac vein; EIA, external iliac artery; EIV, external iliac vein; IIA, internal iliac artery; IIV, internal iliac vein; OA, obturator artery; OV, obturator vein.

The operative scope of the ESS approach. (A) Adjusting the working arm angle allows for a wide range of flexible movement of the surgical instrument within a fan‐shaped area for most patients. (B) Repositioning the port and re‐docking the surgical robot for patients with a higher BMI to access lymph nodes at higher positions.
Similar articles
-
Lymphocele after extraperitoneal robot-assisted radical prostatectomy: a propensity score-matching study.Int J Urol. 2013 Dec;20(12):1169-76. doi: 10.1111/iju.12144. Epub 2013 Mar 21. Int J Urol. 2013. PMID: 23521086
-
The deep vein thrombosis caused by lymphocele after endoscopic extraperitoneal radical prostatectomy and pelvic lymph node dissection.Can Urol Assoc J. 2011 Jun;5(3):E40-3. doi: 10.5489/cuaj.10093. Can Urol Assoc J. 2011. PMID: 21672491 Free PMC article.
-
Standardized comparison of robot-assisted limited and extended pelvic lymphadenectomy for prostate cancer.BJU Int. 2013 Jul;112(1):81-8. doi: 10.1111/j.1464-410X.2012.11788.x. Epub 2013 Jan 25. BJU Int. 2013. PMID: 23351148
-
Role of robot-assisted radical prostatectomy in locally advanced prostate cancer.Int J Urol. 2018 Jan;25(1):30-35. doi: 10.1111/iju.13441. Epub 2017 Sep 13. Int J Urol. 2018. PMID: 28901630 Review.
-
Robot-Assisted Treatment of Symptomatic Lymphocele Postradical Prostatectomy and Lymphadenectomy in the Era or Robotic Surgery: Narrative Review.Technol Cancer Res Treat. 2023 Jan-Dec;22:15330338221145248. doi: 10.1177/15330338221145248. Technol Cancer Res Treat. 2023. PMID: 37350154 Free PMC article. Review.
References
-
- Cornford P, Van Den Bergh RCN, Briers E et al. EAU‐EANM‐ESTRO‐ESUR‐ISUP‐SIOG guidelines on prostate cancer—2024 update. Part I: screening, diagnosis, and local treatment with curative intent. Eur Urol 2024; 86: 148–163 - PubMed
-
- Kaouk J, Aminsharifi A, Wilson CA et al. Extraperitoneal versus transperitoneal single port robotic radical prostatectomy: a comparative analysis of perioperative outcomes. J Urol 2020; 203: 1135–1140 - PubMed
-
- Lenfant L, Sawczyn G, Aminsharifi A et al. Pure single‐site robot‐assisted radical prostatectomy using single‐port versus multiport robotic radical prostatectomy: a single‐institution comparative study. Eur Urol Focus 2021; 7: 964–972 - PubMed
-
- Ploussard G, Briganti A, De La Taille A et al. Pelvic lymph node dissection during robot‐assisted radical prostatectomy: efficacy, limitations, and complications—a systematic review of the literature. Eur Urol 2014; 65: 7–16 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
